Authorization For Release Of Information Form - I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I give permission to release the health information of: Atrium health teammate name & department.
The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. I give permission to release the health information of: Atrium health teammate name & department.
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I give permission to release the health information of: Atrium health teammate name & department.
Consent Release Medical Information Form Fill Out And vrogue.co
I give permission to release the health information of: Atrium health teammate name & department. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164;
FREE 13+ Sample Release of Information Forms in PDF MS Word
Atrium health teammate name & department. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I give permission to release the health information of: I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record.
Authorization For Release Of Information Form Printable Pdf Download
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. I give permission to release the health information of: The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Atrium health teammate name & department.

Authorization to Release Information Fill Out, Sign Online and
I give permission to release the health information of: Atrium health teammate name & department. I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164;
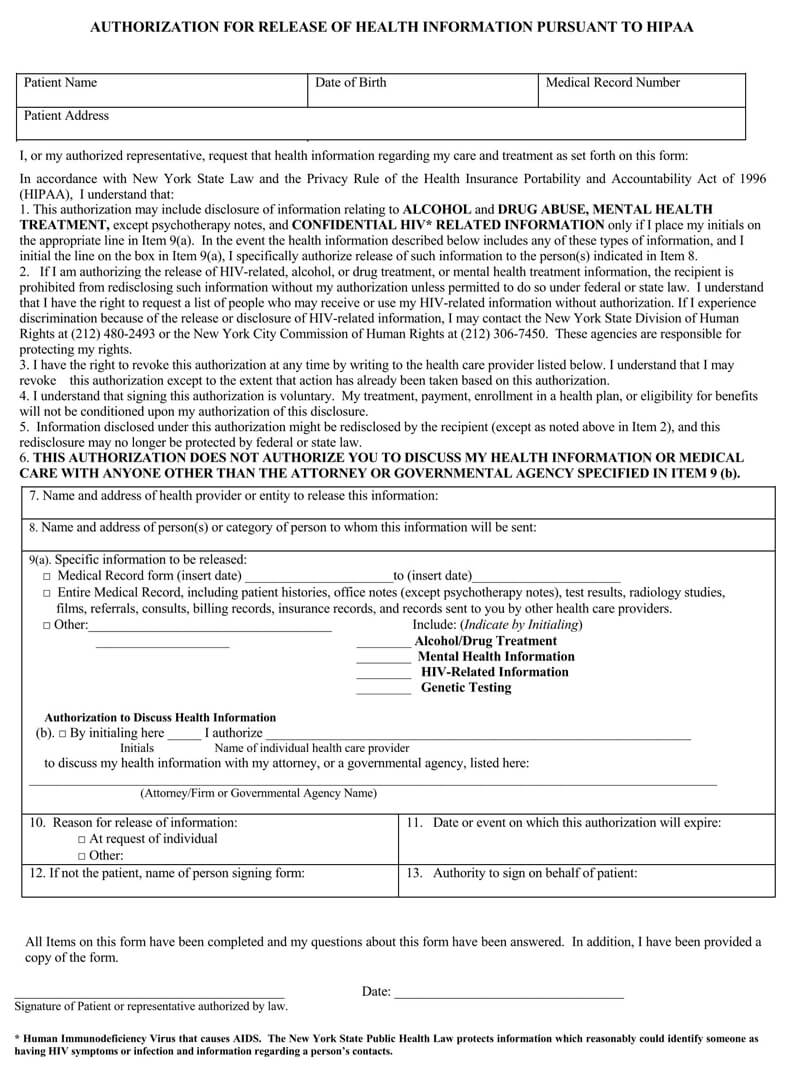
Authorization for Release of Information Authorization Release
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Atrium health teammate name & department. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I give permission to release the health information of:
FREE 13+ Sample Release of Information Forms in PDF MS Word
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Atrium health teammate name & department. I give permission to release the health information of: The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164;

Consent To Release Information Form Template Printable Word Searches
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Atrium health teammate name & department. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I give permission to release the health information of:
Release of Information Consent Form Template for Private Etsy Australia
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I give permission to release the health information of: Atrium health teammate name & department.
Printable Blank Authorization To Release Information Form Printable
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Atrium health teammate name & department. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I give permission to release the health information of:

Release of Information Form 5 Free Templates in PDF, Word, Excel Download
I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Atrium health teammate name & department. I give permission to release the health information of: The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164;
I Give Permission To Release The Health Information Of:
The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; I, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Atrium health teammate name & department.