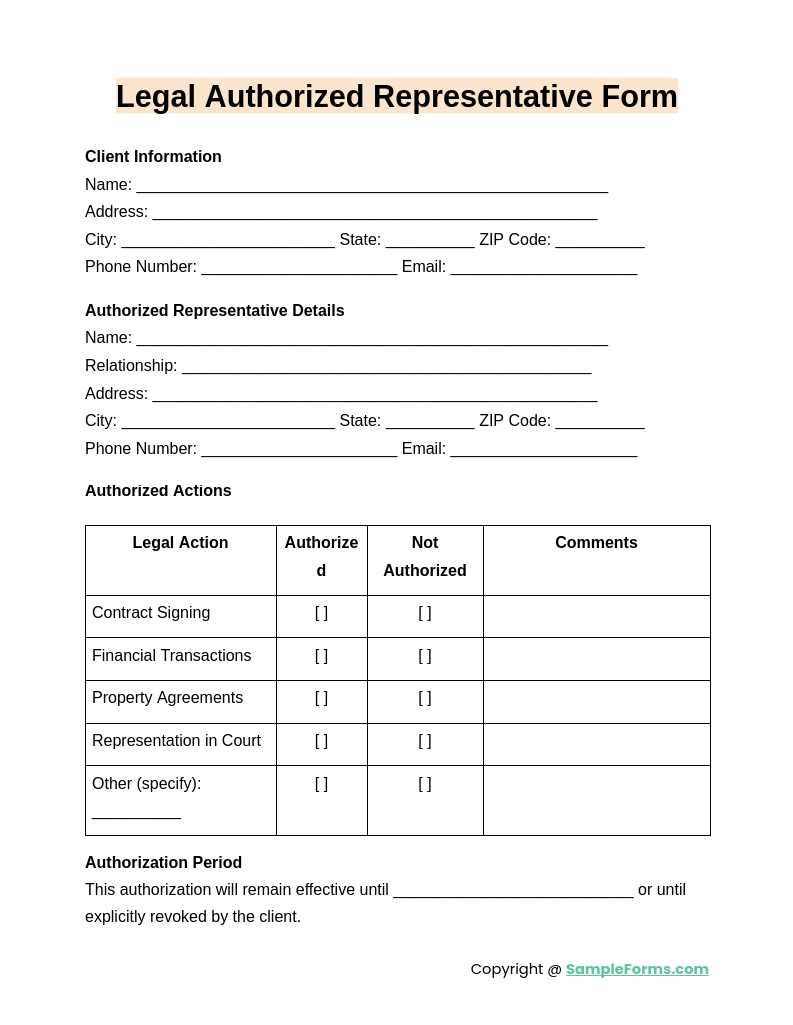
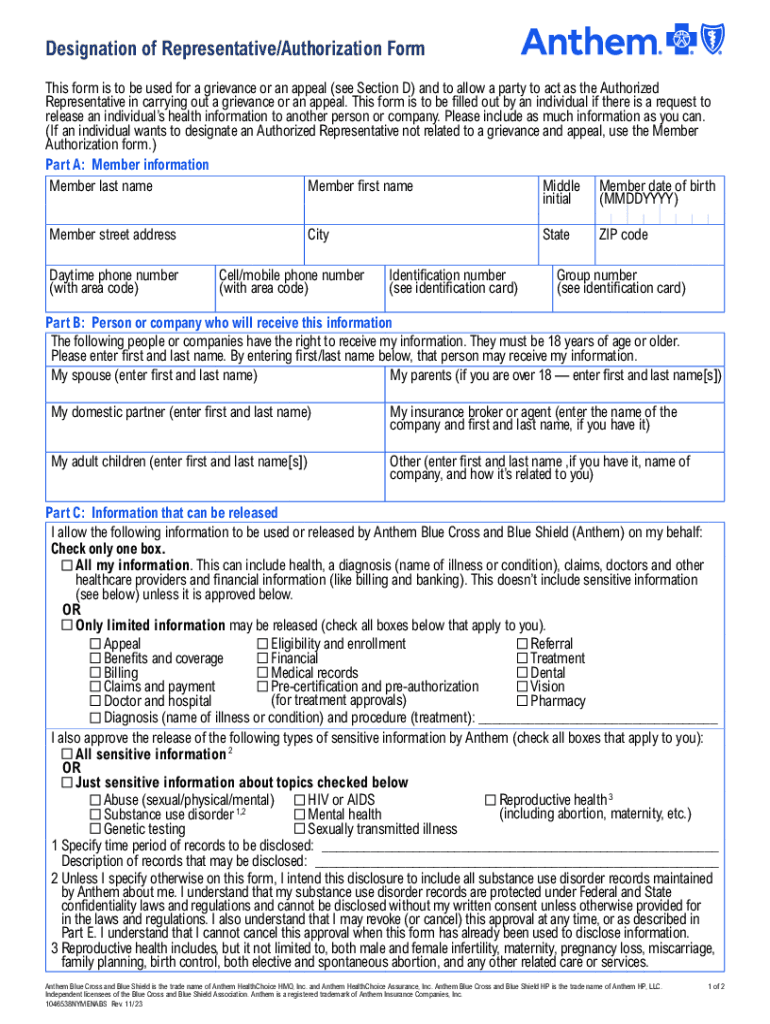
Authorized Rep Form - If you want to name a person or. _________________________________________________________ to act as my authorized representative. This individual is an adult who is sufficiently aware of. Appointment of representative use this form to appoint a representative to act on your behalf for your claim, appeal, grievance or request. If you decide to appoint someone to help you with your case, you must tell us in writing. Understand that if the person approved to receive the information is not a health. You have the right to appoint an authorized representative to act on your behalf with the department. You can sign and submit a written statement appointing the. Withdrawing consent given to a legal representative will be verified.
You have the right to appoint an authorized representative to act on your behalf with the department. Appointment of representative use this form to appoint a representative to act on your behalf for your claim, appeal, grievance or request. Withdrawing consent given to a legal representative will be verified. Understand that if the person approved to receive the information is not a health. _________________________________________________________ to act as my authorized representative. If you want to name a person or. This individual is an adult who is sufficiently aware of. If you decide to appoint someone to help you with your case, you must tell us in writing. You can sign and submit a written statement appointing the.
Appointment of representative use this form to appoint a representative to act on your behalf for your claim, appeal, grievance or request. _________________________________________________________ to act as my authorized representative. You have the right to appoint an authorized representative to act on your behalf with the department. If you want to name a person or. Withdrawing consent given to a legal representative will be verified. This individual is an adult who is sufficiently aware of. If you decide to appoint someone to help you with your case, you must tell us in writing. You can sign and submit a written statement appointing the. Understand that if the person approved to receive the information is not a health.

Authorized Representative Form Calfresh
If you decide to appoint someone to help you with your case, you must tell us in writing. If you want to name a person or. Withdrawing consent given to a legal representative will be verified. You have the right to appoint an authorized representative to act on your behalf with the department. You can sign and submit a written.
FREE 13+ Authorized Representative Forms Samples, PDF, MS Word, Google Docs
Understand that if the person approved to receive the information is not a health. You can sign and submit a written statement appointing the. This individual is an adult who is sufficiently aware of. You have the right to appoint an authorized representative to act on your behalf with the department. Appointment of representative use this form to appoint a.

Authorized representative request Fill out & sign online DocHub
This individual is an adult who is sufficiently aware of. _________________________________________________________ to act as my authorized representative. If you want to name a person or. Understand that if the person approved to receive the information is not a health. If you decide to appoint someone to help you with your case, you must tell us in writing.
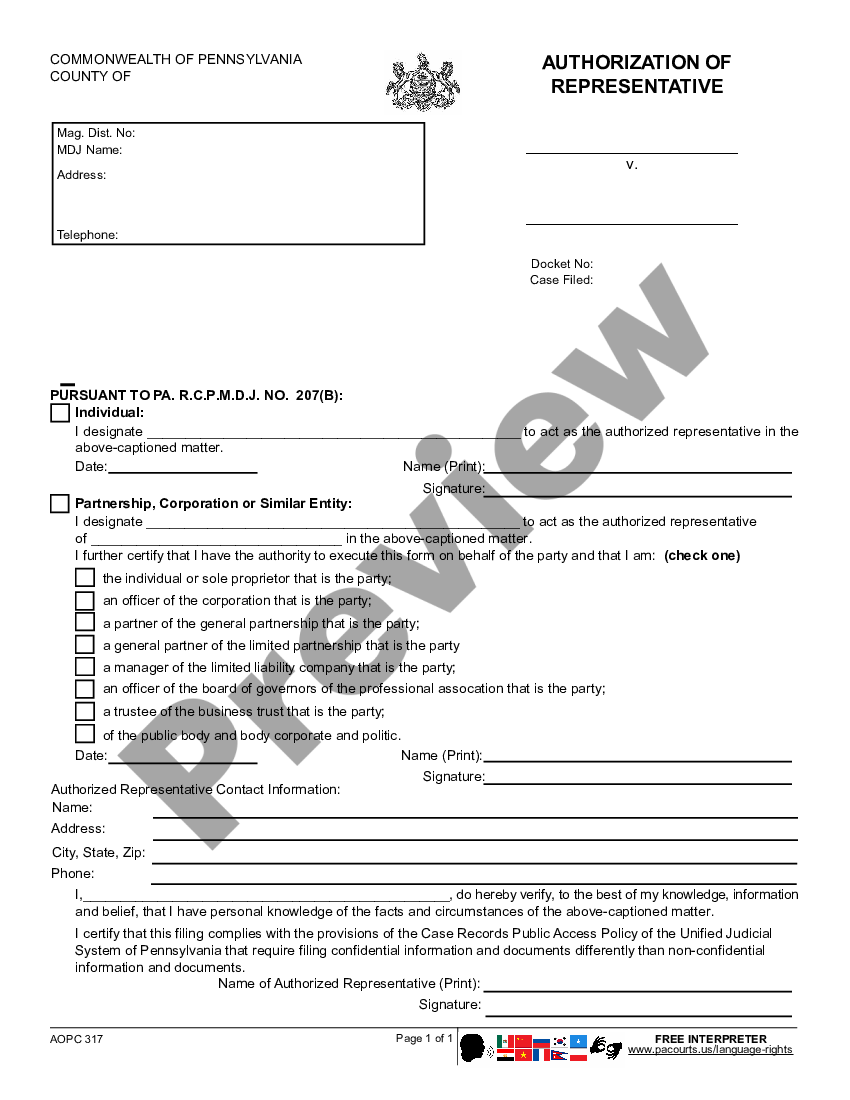
Pennsylvania Authorization of Representative Authorization Of
Appointment of representative use this form to appoint a representative to act on your behalf for your claim, appeal, grievance or request. This individual is an adult who is sufficiently aware of. If you decide to appoint someone to help you with your case, you must tell us in writing. If you want to name a person or. _________________________________________________________ to.
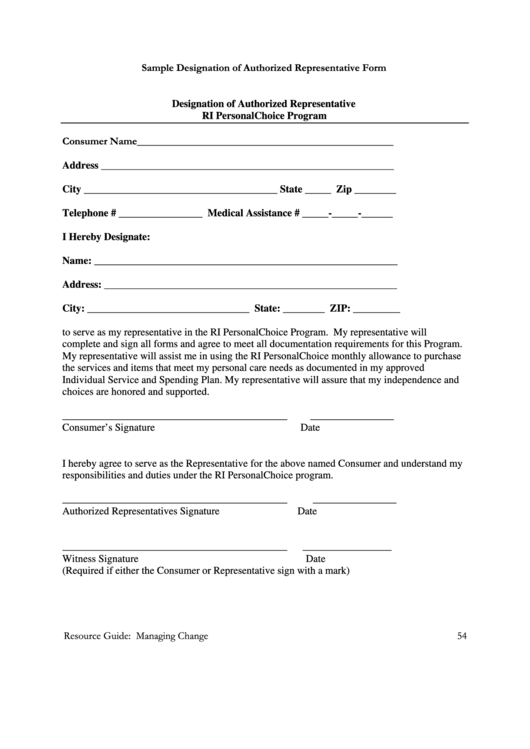
Sample Designation Of Authorized Representative Form Printable Pdf
Understand that if the person approved to receive the information is not a health. You can sign and submit a written statement appointing the. Appointment of representative use this form to appoint a representative to act on your behalf for your claim, appeal, grievance or request. Withdrawing consent given to a legal representative will be verified. _________________________________________________________ to act as.
FREE 13+ Authorized Representative Forms Samples, PDF, MS Word, Google Docs
You have the right to appoint an authorized representative to act on your behalf with the department. Understand that if the person approved to receive the information is not a health. You can sign and submit a written statement appointing the. Appointment of representative use this form to appoint a representative to act on your behalf for your claim, appeal,.
Fillable Online Instructions for completing the Designation of
This individual is an adult who is sufficiently aware of. _________________________________________________________ to act as my authorized representative. If you decide to appoint someone to help you with your case, you must tell us in writing. You have the right to appoint an authorized representative to act on your behalf with the department. Withdrawing consent given to a legal representative will.

Appointment Authorized Representative Fill Online, Printable
If you want to name a person or. You have the right to appoint an authorized representative to act on your behalf with the department. Understand that if the person approved to receive the information is not a health. Withdrawing consent given to a legal representative will be verified. If you decide to appoint someone to help you with your.
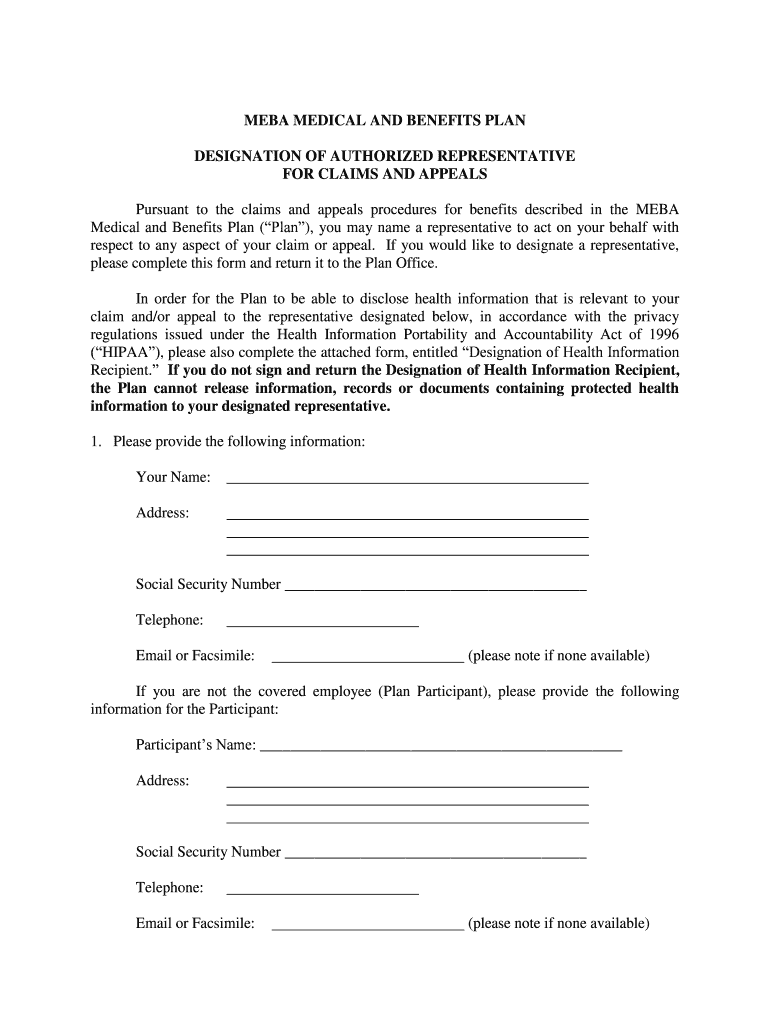
MEBA Medical Plan Designation of Authorized Representative Form Fill
_________________________________________________________ to act as my authorized representative. Withdrawing consent given to a legal representative will be verified. Appointment of representative use this form to appoint a representative to act on your behalf for your claim, appeal, grievance or request. If you decide to appoint someone to help you with your case, you must tell us in writing. Understand that if.

Authorized Rep Form For Medicaid
You can sign and submit a written statement appointing the. Withdrawing consent given to a legal representative will be verified. You have the right to appoint an authorized representative to act on your behalf with the department. _________________________________________________________ to act as my authorized representative. Understand that if the person approved to receive the information is not a health.
You Can Sign And Submit A Written Statement Appointing The.
Appointment of representative use this form to appoint a representative to act on your behalf for your claim, appeal, grievance or request. You have the right to appoint an authorized representative to act on your behalf with the department. If you want to name a person or. _________________________________________________________ to act as my authorized representative.
This Individual Is An Adult Who Is Sufficiently Aware Of.
If you decide to appoint someone to help you with your case, you must tell us in writing. Understand that if the person approved to receive the information is not a health. Withdrawing consent given to a legal representative will be verified.