Coordination Of Benefits Form - Was another party, defective product or a motor. Do you and/or another family member have medicare? To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). Are you or any member of your family covered under any other health insurance or medicare? The bcrc takes actions to identify the health benefits available to a beneficiary and coordinates the payment process to prevent. If yes, provide the following for each family member with medicare. If there is coverage through another healthcare plan, excluding medicare and auto insurance, you can update your coordination of benefits information.
The bcrc takes actions to identify the health benefits available to a beneficiary and coordinates the payment process to prevent. To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). Do you and/or another family member have medicare? Are you or any member of your family covered under any other health insurance or medicare? Was another party, defective product or a motor. If yes, provide the following for each family member with medicare. If there is coverage through another healthcare plan, excluding medicare and auto insurance, you can update your coordination of benefits information.
The bcrc takes actions to identify the health benefits available to a beneficiary and coordinates the payment process to prevent. Are you or any member of your family covered under any other health insurance or medicare? If yes, provide the following for each family member with medicare. If there is coverage through another healthcare plan, excluding medicare and auto insurance, you can update your coordination of benefits information. Do you and/or another family member have medicare? To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). Was another party, defective product or a motor.
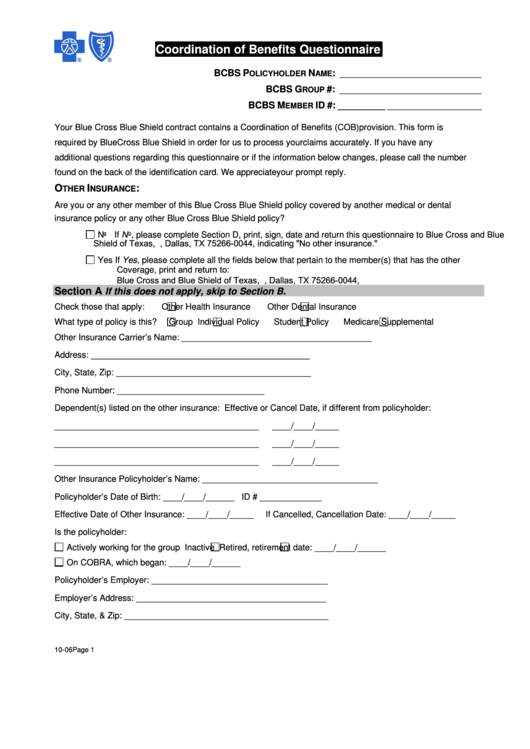
Fillable Bcbs Coordination Of Benefits Questionnaire printable pdf download
Are you or any member of your family covered under any other health insurance or medicare? Was another party, defective product or a motor. Do you and/or another family member have medicare? To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). The bcrc takes actions to identify.
Coordination of benefits letter Fill out & sign online DocHub
The bcrc takes actions to identify the health benefits available to a beneficiary and coordinates the payment process to prevent. If there is coverage through another healthcare plan, excluding medicare and auto insurance, you can update your coordination of benefits information. To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim,.
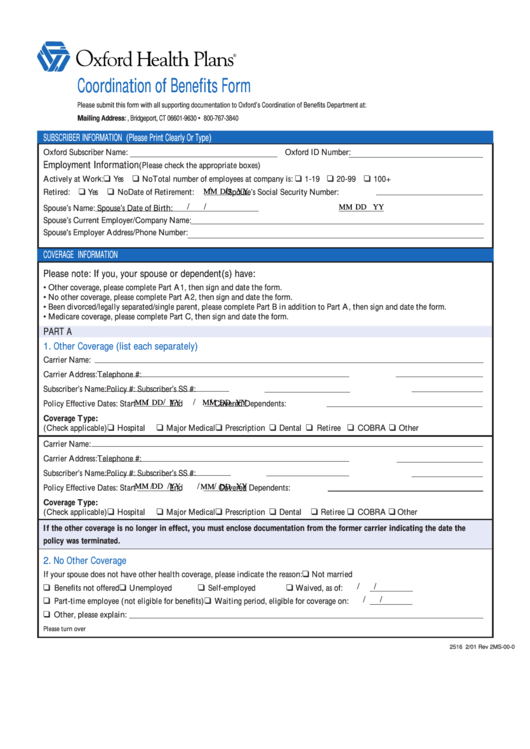
Fillable Coordination Of Benefits Form printable pdf download
Was another party, defective product or a motor. To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). The bcrc takes actions to identify the health benefits available to a beneficiary and coordinates the payment process to prevent. If yes, provide the following for each family member with.

Fillable Online pibf COORDINATION OF BENEFITS FORM Fax
Do you and/or another family member have medicare? If yes, provide the following for each family member with medicare. The bcrc takes actions to identify the health benefits available to a beneficiary and coordinates the payment process to prevent. Are you or any member of your family covered under any other health insurance or medicare? Was another party, defective product.
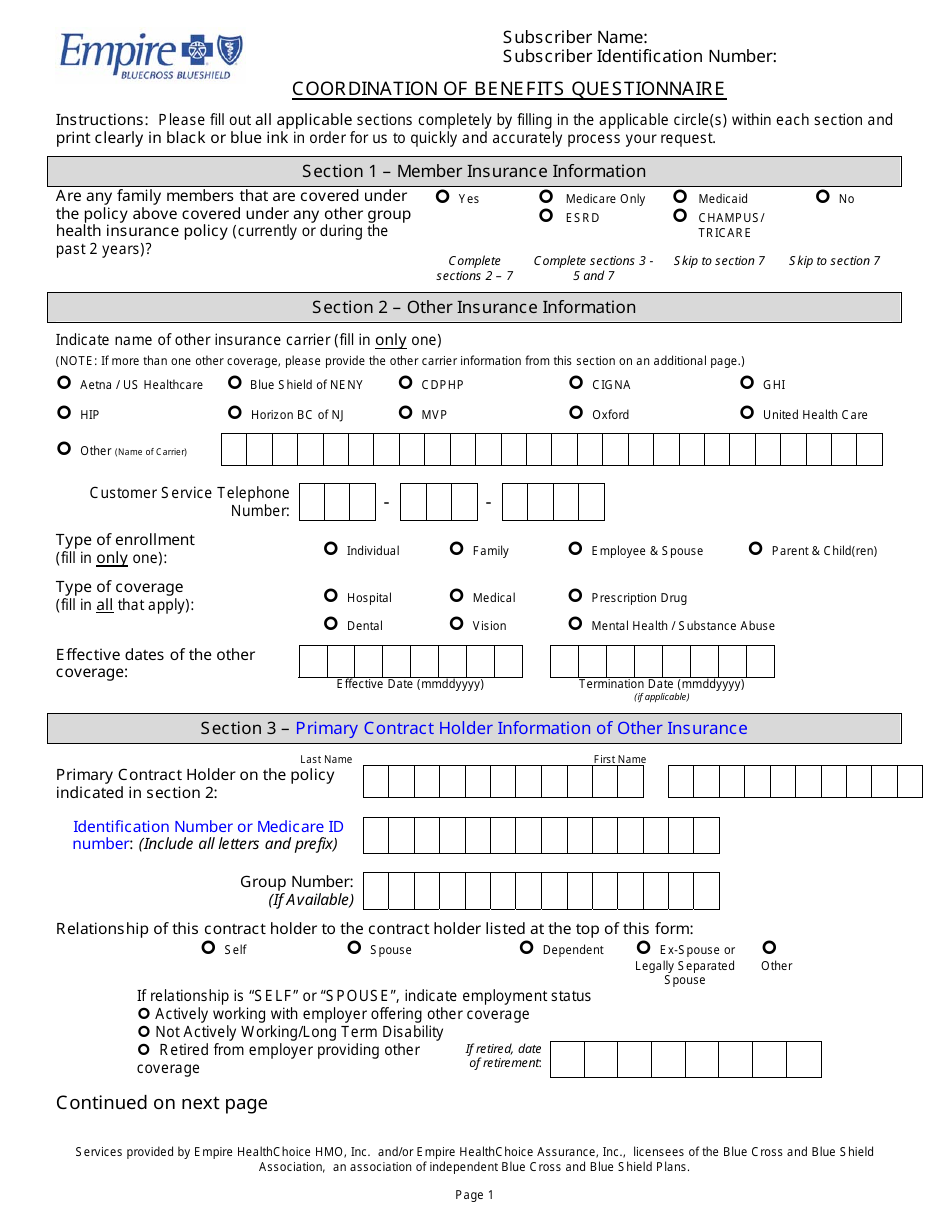
Coordination of Benefits Questionnaire Form Empire Blue Cross Blue
Was another party, defective product or a motor. To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). If there is coverage through another healthcare plan, excluding medicare and auto insurance, you can update your coordination of benefits information. The bcrc takes actions to identify the health benefits.

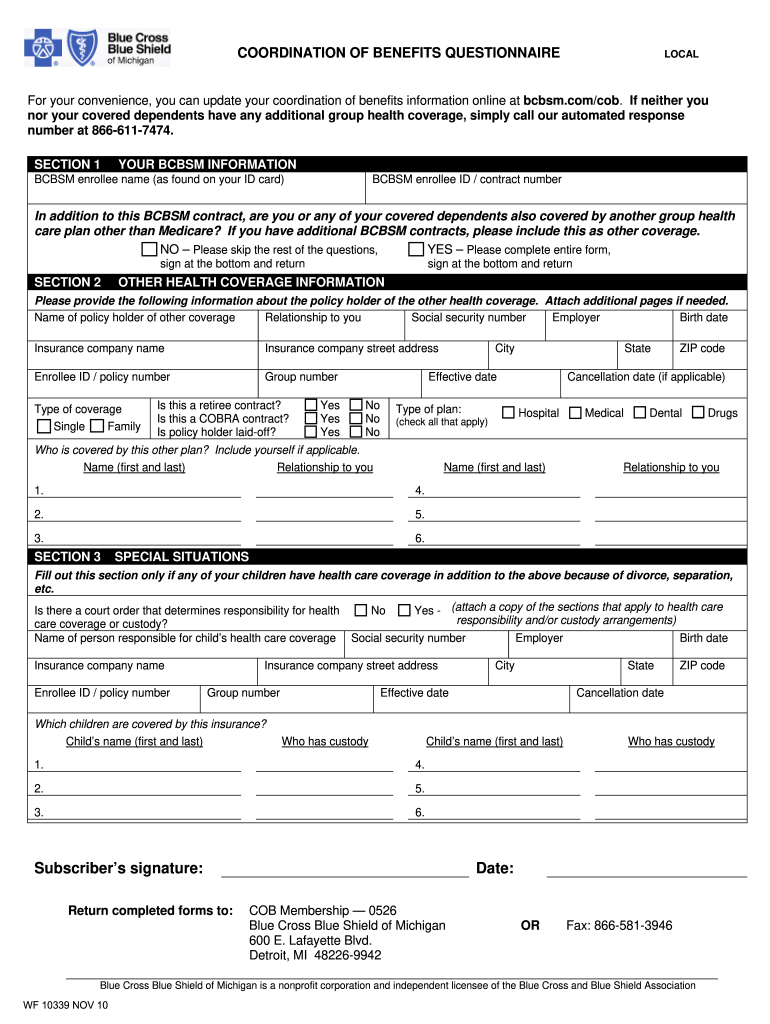
Coordination of Benefits Questionnaire PDF Insurance Medicare
Do you and/or another family member have medicare? Are you or any member of your family covered under any other health insurance or medicare? If there is coverage through another healthcare plan, excluding medicare and auto insurance, you can update your coordination of benefits information. Was another party, defective product or a motor. To facilitate a quicker response to your.
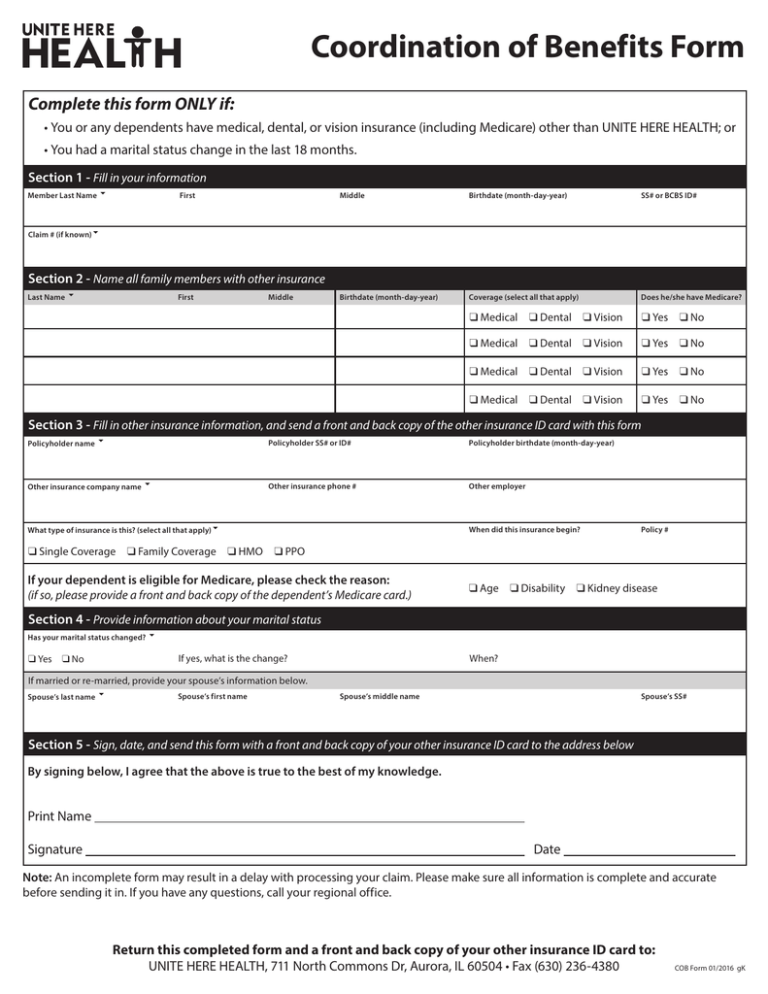
0116Form Coordination of Benefits.indd
Was another party, defective product or a motor. Are you or any member of your family covered under any other health insurance or medicare? To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). If there is coverage through another healthcare plan, excluding medicare and auto insurance, you.

Coordination of Benefits Medical Includes Vision Dental RX Group
To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). Are you or any member of your family covered under any other health insurance or medicare? Do you and/or another family member have medicare? The bcrc takes actions to identify the health benefits available to a beneficiary and.
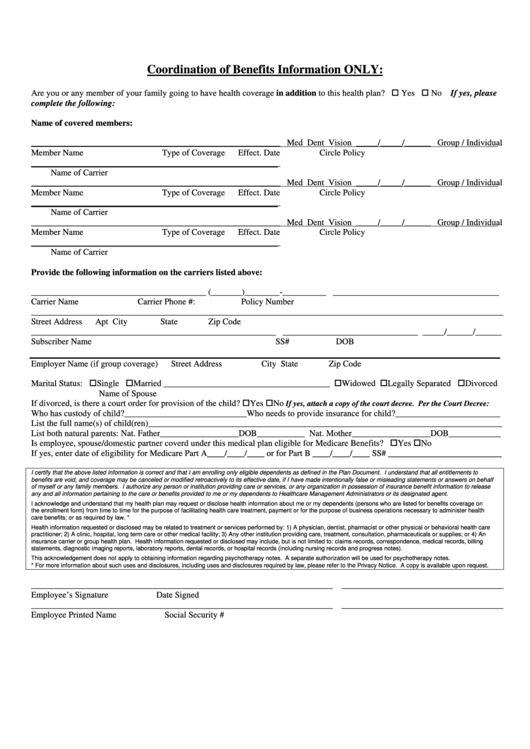
Coordination Of Benefits Information printable pdf download
Are you or any member of your family covered under any other health insurance or medicare? If yes, provide the following for each family member with medicare. To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes). If there is coverage through another healthcare plan, excluding medicare and.
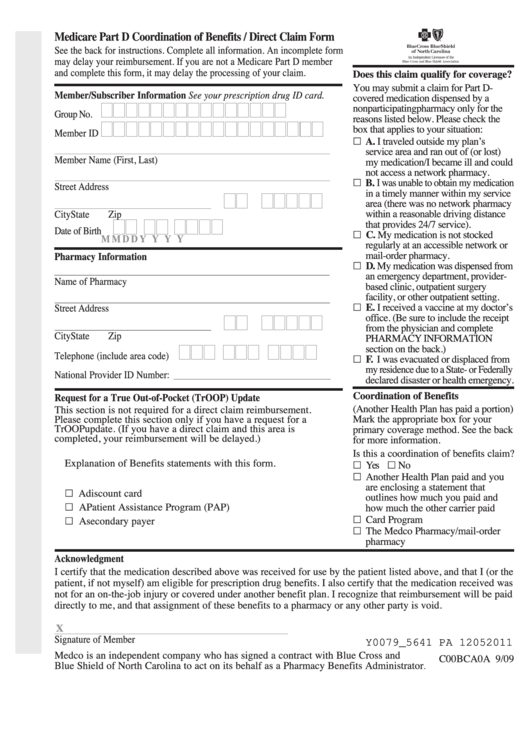
Fillable Medicare Part D Coordination Of Benefits Direct Claim Form
If there is coverage through another healthcare plan, excluding medicare and auto insurance, you can update your coordination of benefits information. Was another party, defective product or a motor. The bcrc takes actions to identify the health benefits available to a beneficiary and coordinates the payment process to prevent. If yes, provide the following for each family member with medicare..
If Yes, Provide The Following For Each Family Member With Medicare.
The bcrc takes actions to identify the health benefits available to a beneficiary and coordinates the payment process to prevent. Are you or any member of your family covered under any other health insurance or medicare? Do you and/or another family member have medicare? To facilitate a quicker response to your inquiry, please complete this form and attach all relevant claim information (claim, eomb, operative notes).
Was Another Party, Defective Product Or A Motor.
If there is coverage through another healthcare plan, excluding medicare and auto insurance, you can update your coordination of benefits information.