Dupixent Asthma Enrollment Form - If enrolling in the dupixent myway copay card program, i understand that copay card information will be sent to my designated specialty pharmacy. My signature certifies that the person named on this form is my patient; If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. The information provided on this application, to the best of my knowledge, is. Please provide us with your email address to receive email communications. I understand that my patient’s information provided to regeneron. Choose the appropriate form below and complete the required fields.
If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. I understand that my patient’s information provided to regeneron. Choose the appropriate form below and complete the required fields. If enrolling in the dupixent myway copay card program, i understand that copay card information will be sent to my designated specialty pharmacy. My signature certifies that the person named on this form is my patient; The information provided on this application, to the best of my knowledge, is. Please provide us with your email address to receive email communications.
Choose the appropriate form below and complete the required fields. I understand that my patient’s information provided to regeneron. If enrolling in the dupixent myway copay card program, i understand that copay card information will be sent to my designated specialty pharmacy. My signature certifies that the person named on this form is my patient; The information provided on this application, to the best of my knowledge, is. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Please provide us with your email address to receive email communications.
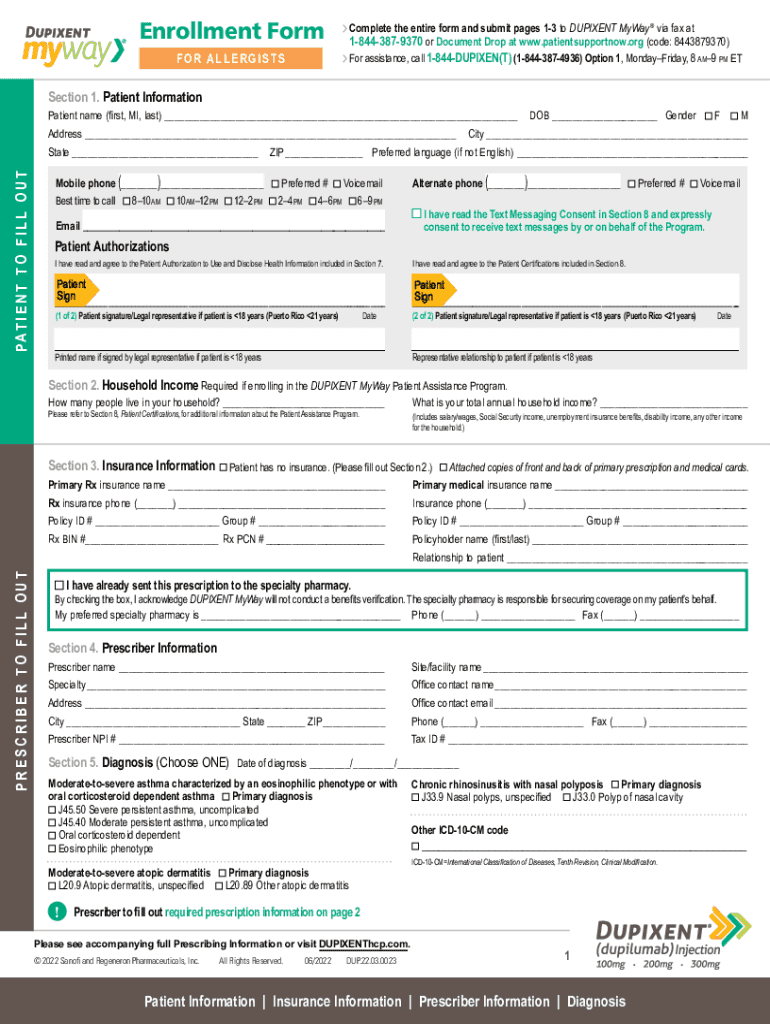
Fillable Online Dupixent Myway Enrollment Form AsthmaNoddem Fax Email
If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. My signature certifies that the person named on this form is my patient; If enrolling in the dupixent myway copay card program, i understand that copay card information will be sent to my designated specialty pharmacy..

Dupixent Myway Enrollment Forms Form example download
I understand that my patient’s information provided to regeneron. My signature certifies that the person named on this form is my patient; Choose the appropriate form below and complete the required fields. Please provide us with your email address to receive email communications. If enrolling in the dupixent myway copay card program, i understand that copay card information will be.

Fillable Online Exception Drug Status (EDS) Request Form Dupixent
If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. My signature certifies that the person named on this form is my patient; The information provided on this application, to the best of my knowledge, is. If enrolling in the dupixent myway copay card program, i.
Dupixent Medicare Part D Assistance ReEnroll Form
The information provided on this application, to the best of my knowledge, is. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Choose the appropriate form below and complete the required fields. My signature certifies that the person named on this form is my patient;.
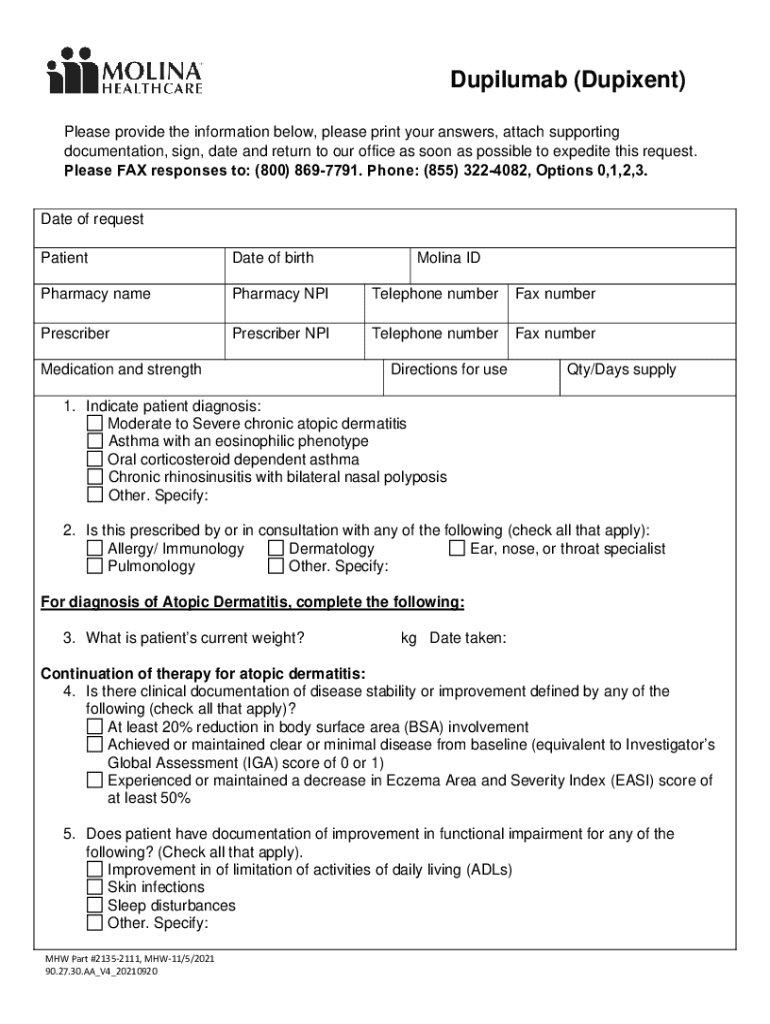
Fillable Online Dupilumab(Dupixent) PA form Fax Email Print pdfFiller
Please provide us with your email address to receive email communications. Choose the appropriate form below and complete the required fields. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. If enrolling in the dupixent myway copay card program, i understand that copay card information.

Dupixent Enrollment Form PDF Download Fillable Form Now
Please provide us with your email address to receive email communications. My signature certifies that the person named on this form is my patient; The information provided on this application, to the best of my knowledge, is. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during.

Fillable Online Enrollment Form Dupixent Fax Email Print pdfFiller
The information provided on this application, to the best of my knowledge, is. My signature certifies that the person named on this form is my patient; If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Choose the appropriate form below and complete the required fields..
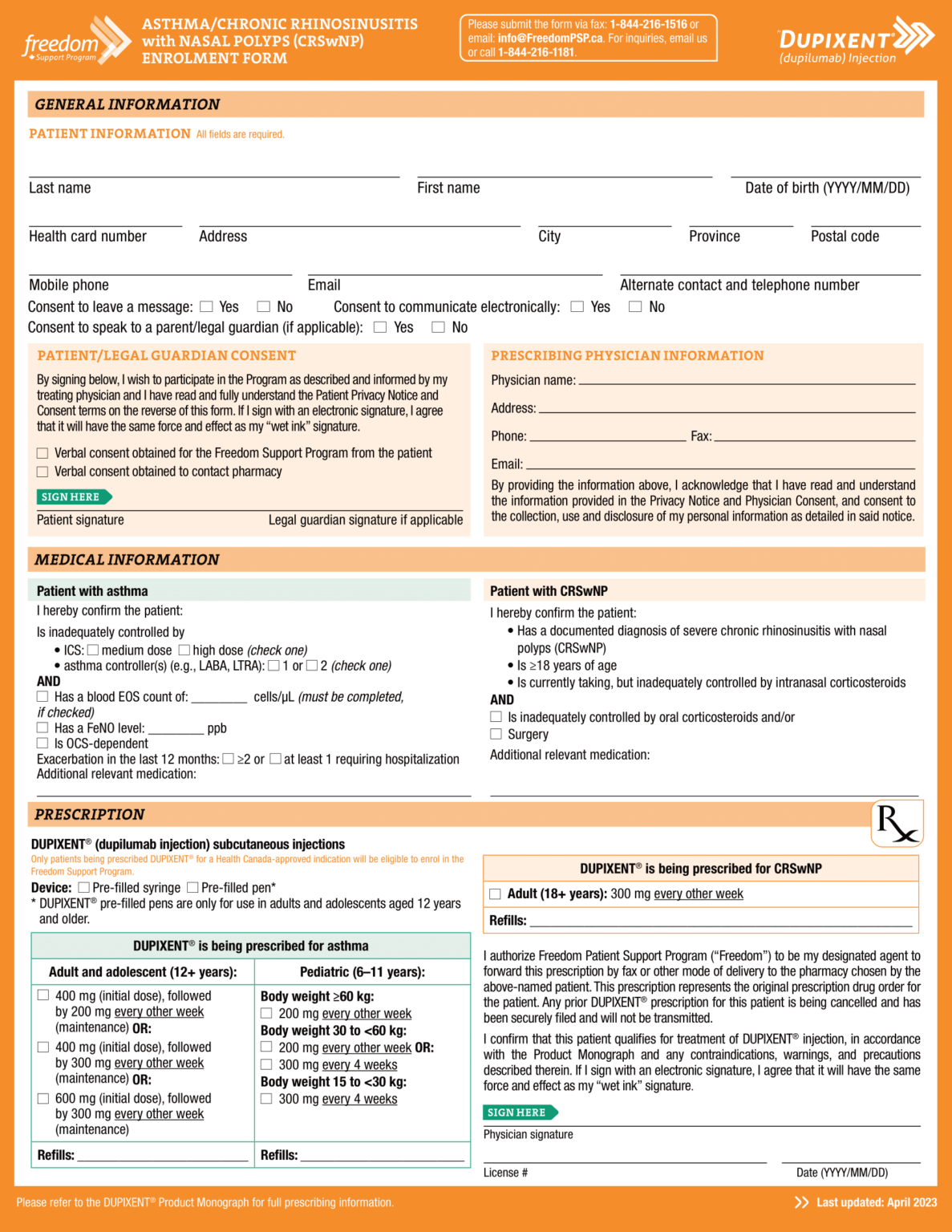
Dupixent (dupilumab) PSP Enrolment Form Asthma CRSwNP EN 2023 World EMR
The information provided on this application, to the best of my knowledge, is. My signature certifies that the person named on this form is my patient; If enrolling in the dupixent myway copay card program, i understand that copay card information will be sent to my designated specialty pharmacy. I understand that my patient’s information provided to regeneron. If i.

Fillable Online Page 1 Specialty Enrollment Form Dupixent Fax Email
I understand that my patient’s information provided to regeneron. If enrolling in the dupixent myway copay card program, i understand that copay card information will be sent to my designated specialty pharmacy. Please provide us with your email address to receive email communications. If i am completing section 5b, i authorize for my commercially insured patient one or more months.

Fillable Online Enrollment Form DUPIXENT Fax Email Print pdfFiller
The information provided on this application, to the best of my knowledge, is. My signature certifies that the person named on this form is my patient; If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Choose the appropriate form below and complete the required fields..
The Information Provided On This Application, To The Best Of My Knowledge, Is.
If enrolling in the dupixent myway copay card program, i understand that copay card information will be sent to my designated specialty pharmacy. Please provide us with your email address to receive email communications. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Choose the appropriate form below and complete the required fields.
I Understand That My Patient’s Information Provided To Regeneron.
My signature certifies that the person named on this form is my patient;