Dupixent Prurigo Nodularis Enrollment Form - Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described in the program enrollment. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Prurigo nodularis enrolment form support program please submit the form via fax: New york state prescription form. Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado.
Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described in the program enrollment. New york state prescription form. Prurigo nodularis enrolment form support program please submit the form via fax: Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a.
New york state prescription form. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described in the program enrollment. Prurigo nodularis enrolment form support program please submit the form via fax: Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado.
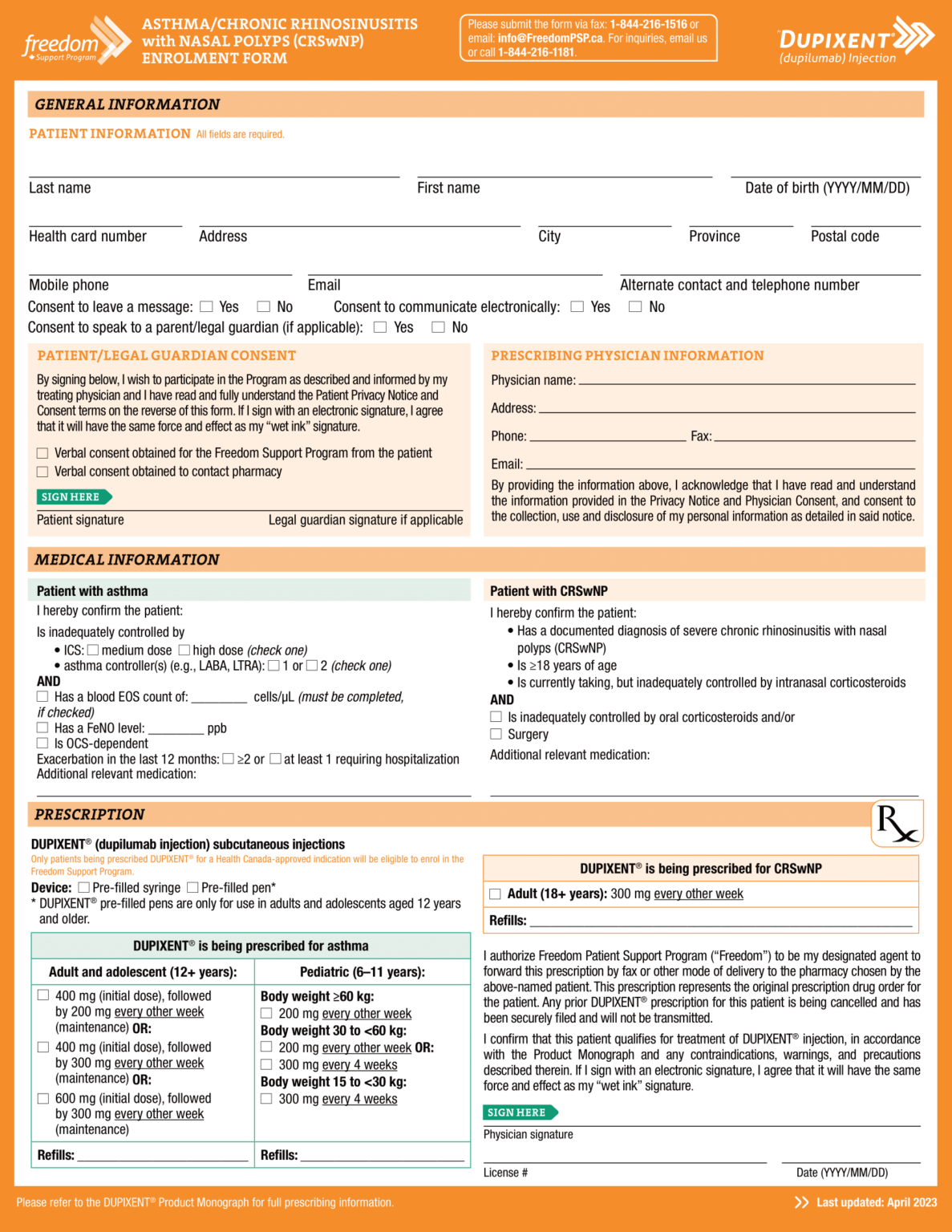
Dupixent (dupilumab) PSP Enrolment Form Asthma CRSwNP EN 2023 World EMR
New york state prescription form. Prurigo nodularis enrolment form support program please submit the form via fax: Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described in the program enrollment. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments.

Dupixent Injection
New york state prescription form. Prurigo nodularis enrolment form support program please submit the form via fax: Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado. If i am completing section 5b, i authorize for my commercially insured patient one or more months.

Dupixent Enrollment Form Fill Online, Printable, Fillable, Blank
If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Prurigo nodularis enrolment form support program please submit the form via fax: Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described in the program enrollment. Autorio.
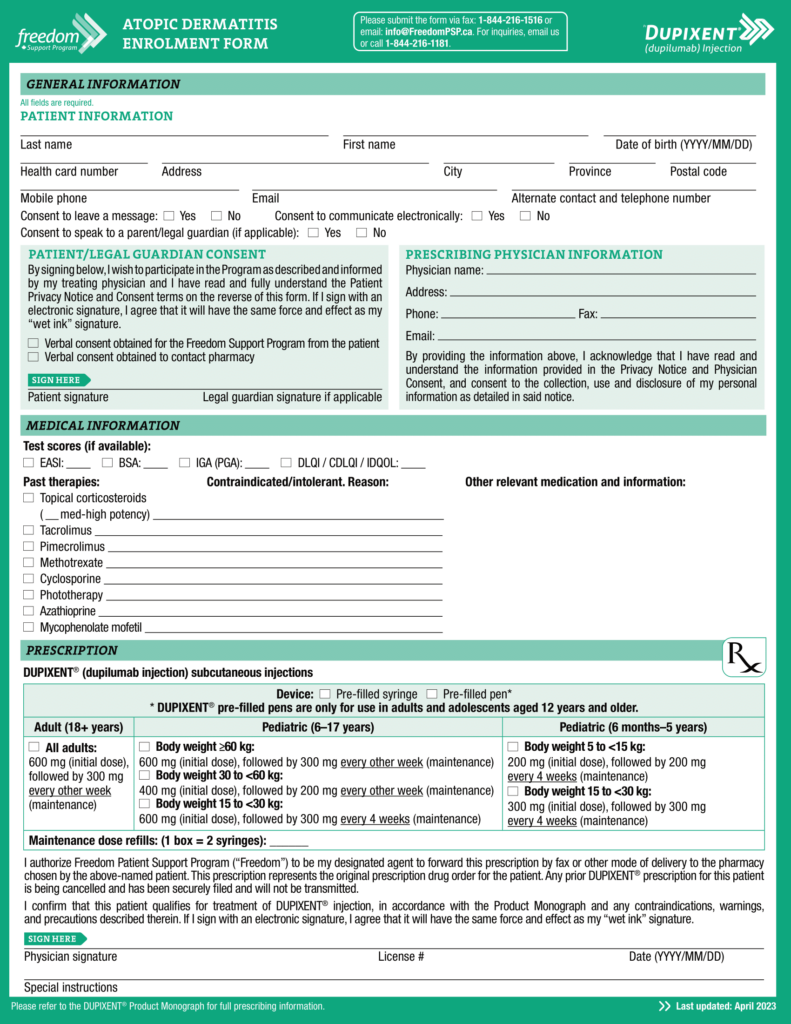
Dupixent (dupilumab) PSP Atopic Derm Enrolment Form CA EN 2023 World EMR
Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Nofi us, and their afiliates and agents (together the “alliance”).
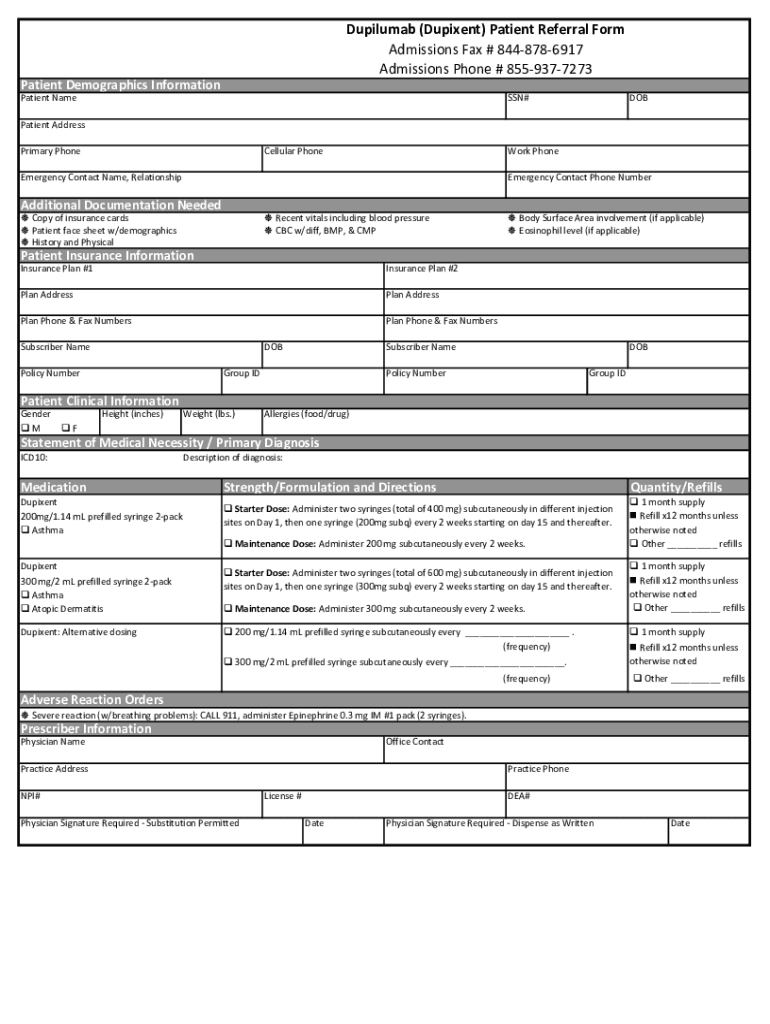
Fillable Online Dupilumab (Dupixent) Patient Referral Form Admissions
Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Nofi us, and their afiliates and agents (together the “alliance”).

Dupixent enrollment form Fill out & sign online DocHub
If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. New york state prescription form. Prurigo nodularis enrolment form support program please submit the form via fax: Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described.

Dupixent Approved for Adults With Prurigo Nodularis MPR
Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado. New york state prescription form. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. Nofi us, and their afiliates.
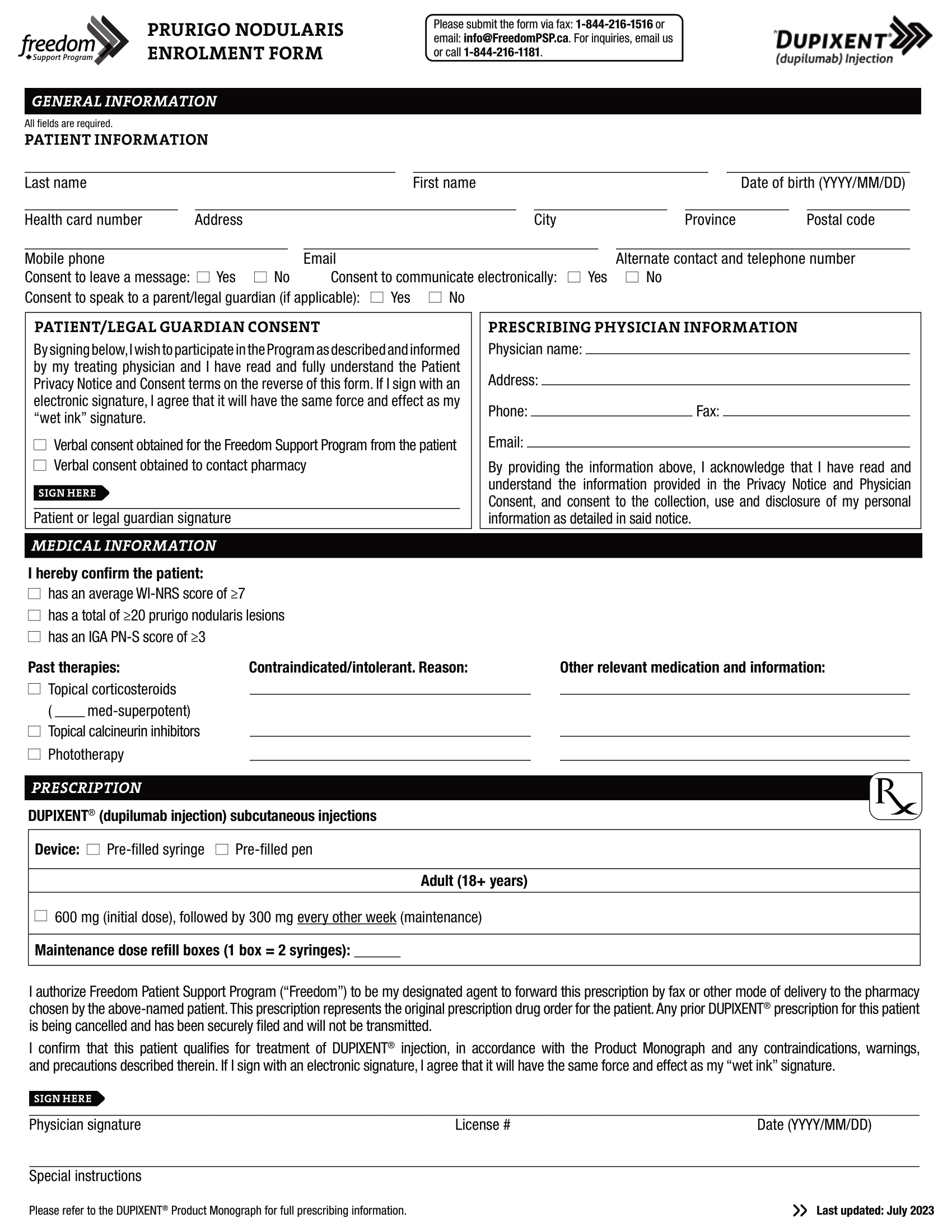
Dupixent (dupilumab) PSP PN Enrolment Form EN 2023 World EMR
Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado. Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described in the program enrollment. Prurigo nodularis enrolment form support program please submit the form via.
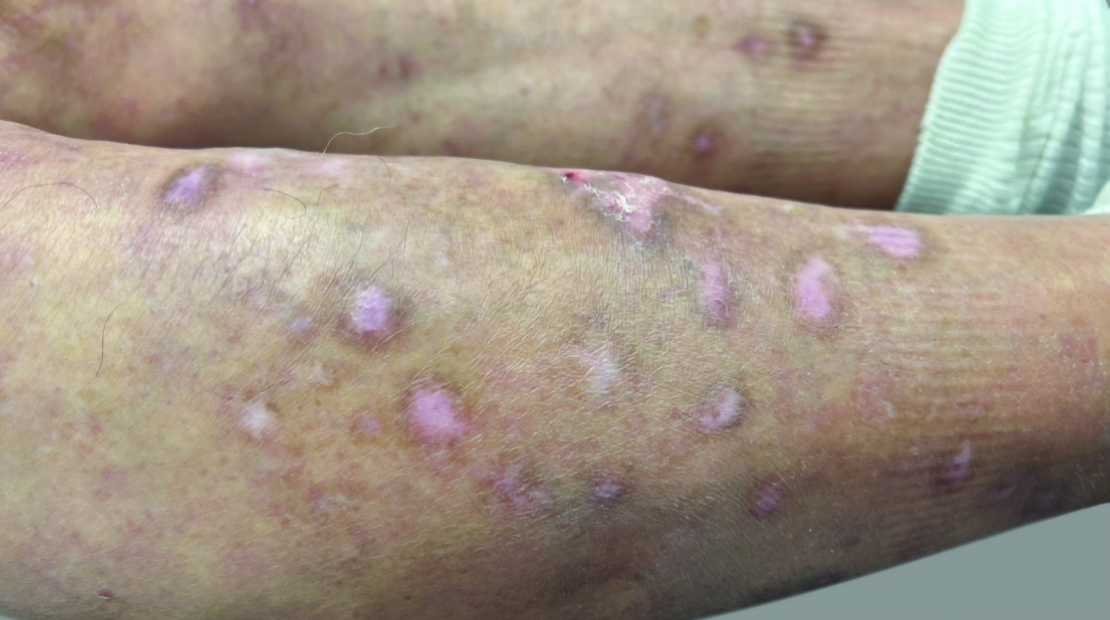
DUPIXENT® (dupilumab) Results in (18+ years)
Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described in the program enrollment. Prurigo nodularis enrolment form support program please submit the form via fax: New york state prescription form. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments.

Fillable Online Enrollment Form Dupixent Fax Email Print pdfFiller
If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a. New york state prescription form. Autorio a ay a enviar esta receta a la farmacia ue le dispense el producto del programa de inicio rpido de dupixent al paciente au mencionado. Prurigo nodularis enrolment form support.
Autorio A Ay A Enviar Esta Receta A La Farmacia Ue Le Dispense El Producto Del Programa De Inicio Rpido De Dupixent Al Paciente Au Mencionado.
Nofi us, and their afiliates and agents (together the “alliance”) to provide me services under the program, as described in the program enrollment. Prurigo nodularis enrolment form support program please submit the form via fax: New york state prescription form. If i am completing section 5b, i authorize for my commercially insured patient one or more months of temporary shipments of dupixent during a.