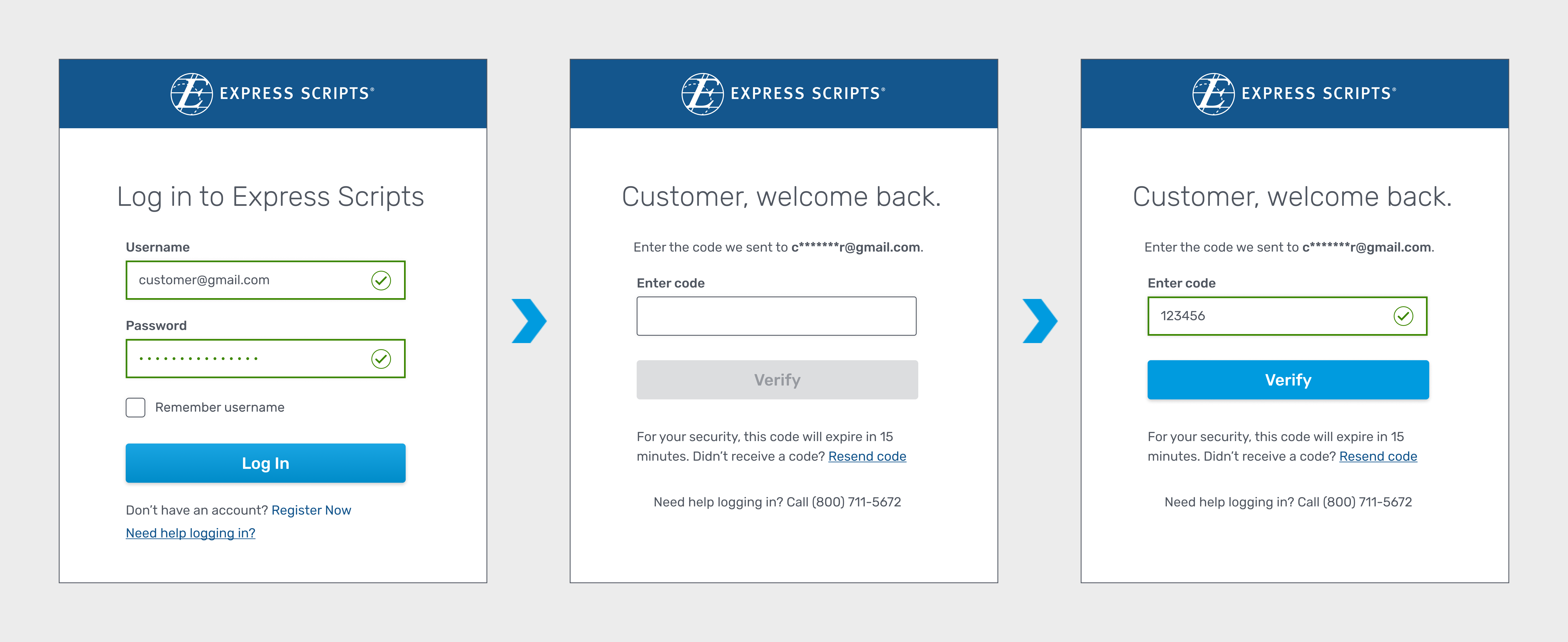
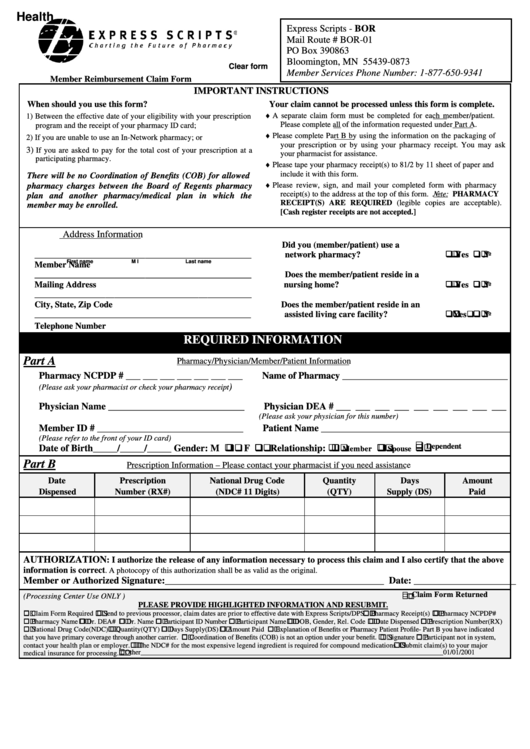
Express Scripts Claim Form - The patient(s) listed below has (have) received the medication, and i authorize release of all information contained on this claim to express scripts, inc. I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. You must submit claims within 1 year of date of purchase or. You must complete a separate claim form for each pharmacy used and for each patient. Now, there are two ways to submit a claim form: Just complete this form and attach the prescription receipt(s) that shows the copayment or coinsurance amount paid at the pharmacy. Complete and submit the form online. It's a secure and quick way to submit your claim.
Complete and submit the form online. The patient(s) listed below has (have) received the medication, and i authorize release of all information contained on this claim to express scripts, inc. Now, there are two ways to submit a claim form: Just complete this form and attach the prescription receipt(s) that shows the copayment or coinsurance amount paid at the pharmacy. I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. You must complete a separate claim form for each pharmacy used and for each patient. You must submit claims within 1 year of date of purchase or. It's a secure and quick way to submit your claim.
It's a secure and quick way to submit your claim. Now, there are two ways to submit a claim form: The patient(s) listed below has (have) received the medication, and i authorize release of all information contained on this claim to express scripts, inc. Complete and submit the form online. You must complete a separate claim form for each pharmacy used and for each patient. Just complete this form and attach the prescription receipt(s) that shows the copayment or coinsurance amount paid at the pharmacy. I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. You must submit claims within 1 year of date of purchase or.
Express Scripts Prior Authorization Form Printable
It's a secure and quick way to submit your claim. You must complete a separate claim form for each pharmacy used and for each patient. Now, there are two ways to submit a claim form: I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. The patient(s).
Prescriber Express Online Fill Online, Printable, Fillable, Blank
I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. Just complete this form and attach the prescription receipt(s) that shows the copayment or coinsurance amount paid at the pharmacy. It's a secure and quick way to submit your claim. The patient(s) listed below has (have) received.
Express Script Pharmacy Prescription Order Form printable pdf download
Complete and submit the form online. You must complete a separate claim form for each pharmacy used and for each patient. It's a secure and quick way to submit your claim. I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. The patient(s) listed below has (have).
Express Scripts Claim Form ≡ Fill Out Printable PDF Forms Online
Complete and submit the form online. You must submit claims within 1 year of date of purchase or. It's a secure and quick way to submit your claim. I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. Now, there are two ways to submit a claim.
Keeping you protected Express Scripts® Pharmacy
You must complete a separate claim form for each pharmacy used and for each patient. The patient(s) listed below has (have) received the medication, and i authorize release of all information contained on this claim to express scripts, inc. Complete and submit the form online. I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree.
Fillable Online Claim Form Express Scripts Fax Email Print pdfFiller
Complete and submit the form online. You must submit claims within 1 year of date of purchase or. Just complete this form and attach the prescription receipt(s) that shows the copayment or coinsurance amount paid at the pharmacy. It's a secure and quick way to submit your claim. You must complete a separate claim form for each pharmacy used and.
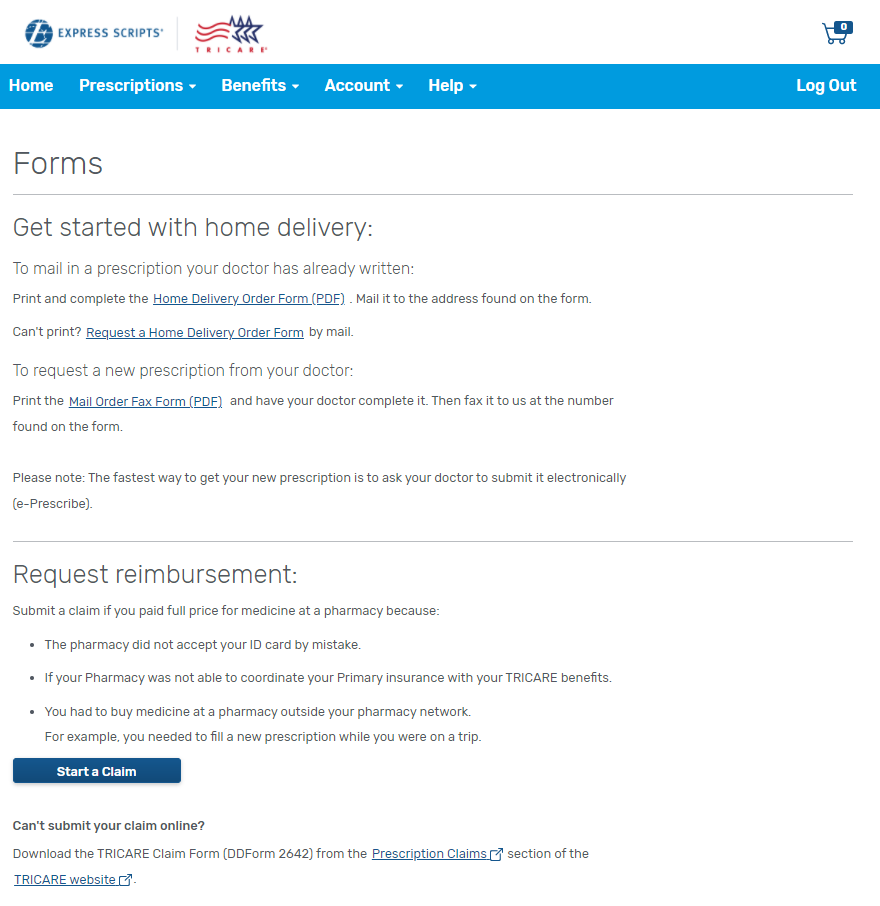
How to file a pharmacy claim online TRICARE Pharmacy Program
You must complete a separate claim form for each pharmacy used and for each patient. It's a secure and quick way to submit your claim. You must submit claims within 1 year of date of purchase or. I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable..

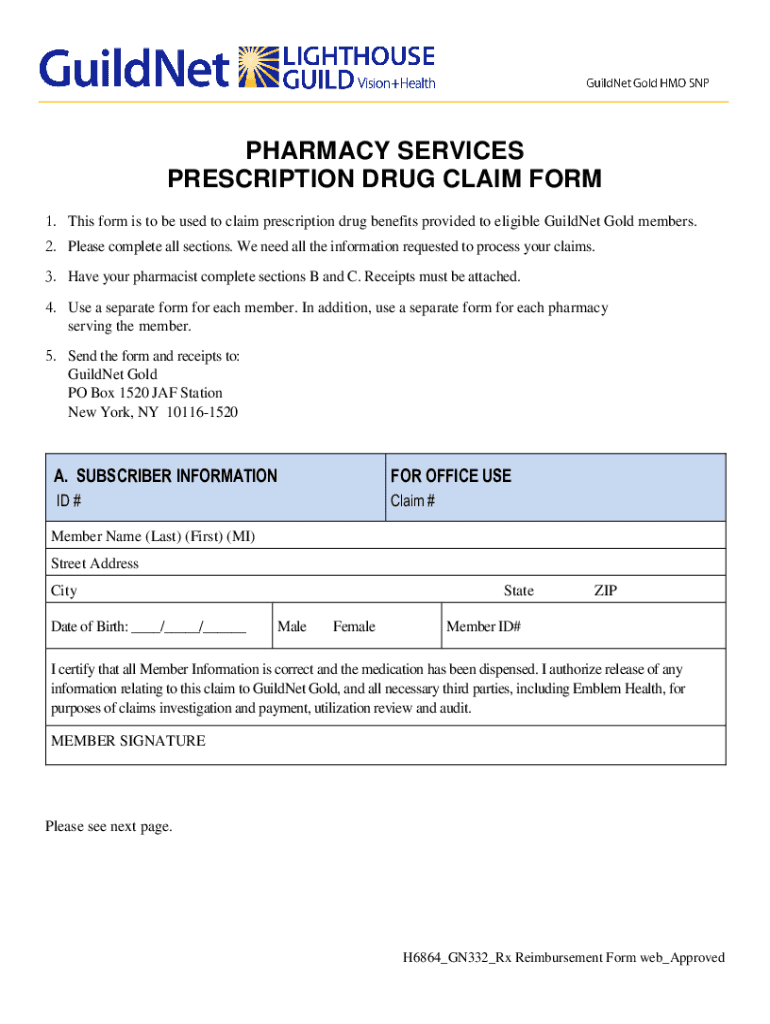
Express Scripts Prescription Drug Claim Form Us PDF Medical
Now, there are two ways to submit a claim form: I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. Just complete this form and attach the prescription receipt(s) that shows the copayment or coinsurance amount paid at the pharmacy. You must complete a separate claim form.
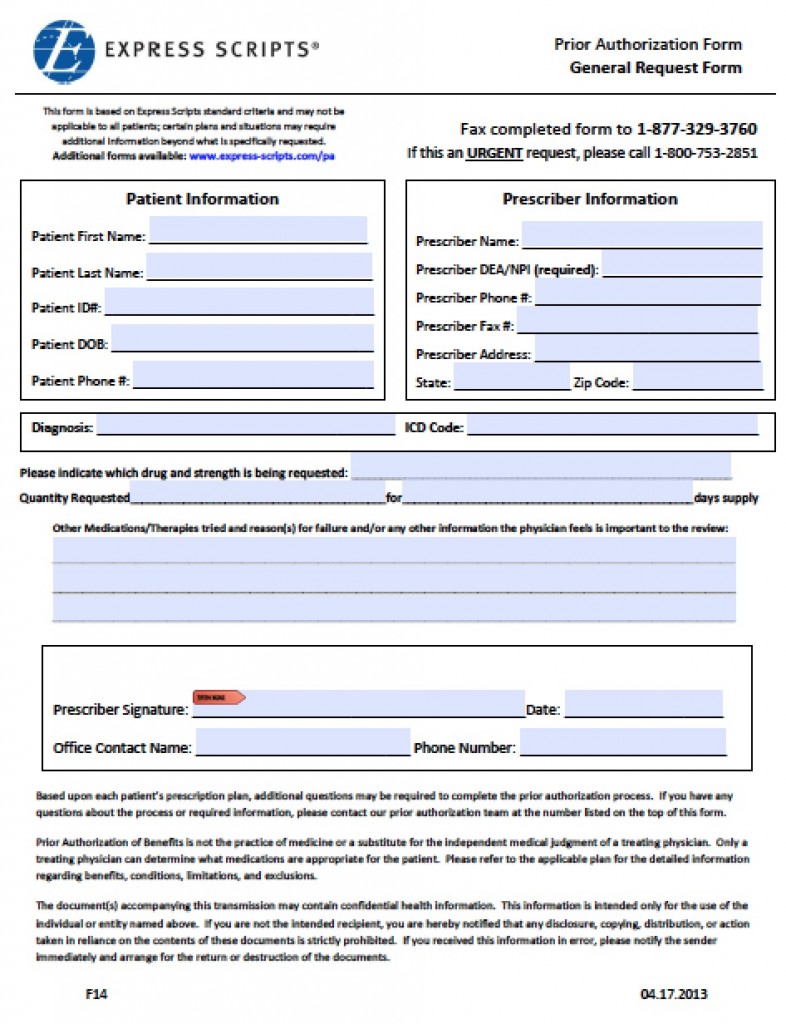
Tricare Express Scripts Prior Auth Form at viiaislinnblog Blog
It's a secure and quick way to submit your claim. Now, there are two ways to submit a claim form: The patient(s) listed below has (have) received the medication, and i authorize release of all information contained on this claim to express scripts, inc. I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to.
Fillable Express Scripts Claim Form printable pdf download
Now, there are two ways to submit a claim form: The patient(s) listed below has (have) received the medication, and i authorize release of all information contained on this claim to express scripts, inc. Just complete this form and attach the prescription receipt(s) that shows the copayment or coinsurance amount paid at the pharmacy. It's a secure and quick way.
You Must Complete A Separate Claim Form For Each Pharmacy Used And For Each Patient.
Now, there are two ways to submit a claim form: I hereby certify that the charge(s) shown for the medication(s) prescribed is correct and agree to provide express scripts or its agents reasonable. You must submit claims within 1 year of date of purchase or. The patient(s) listed below has (have) received the medication, and i authorize release of all information contained on this claim to express scripts, inc.
Just Complete This Form And Attach The Prescription Receipt(S) That Shows The Copayment Or Coinsurance Amount Paid At The Pharmacy.
It's a secure and quick way to submit your claim. Complete and submit the form online.