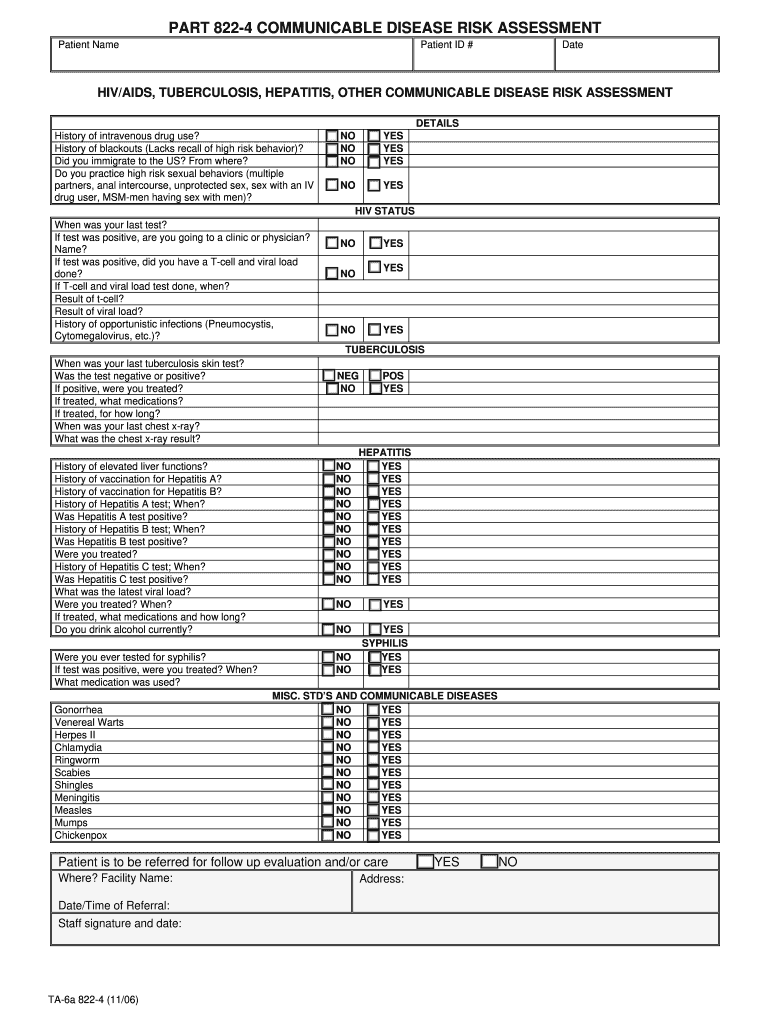
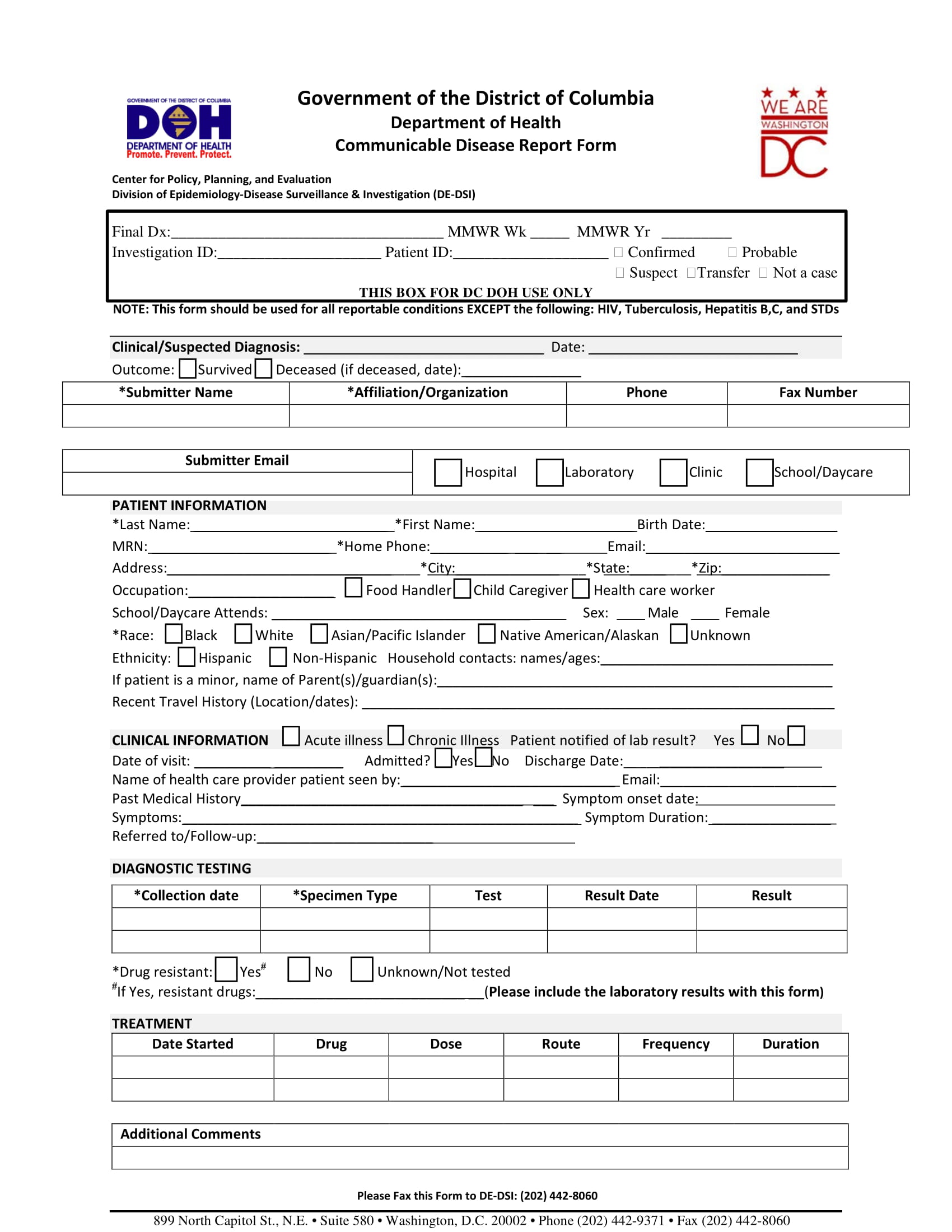
Free Of Communicable Disease Form - Statement of good health/free of communicable disease explanation and instruction: ________________ i have examined _______________________________________, and to. Physician’s statement form date of physical: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. This 9 can be filled in electronically. I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Complete the following information to notify the florida department of health of a reportable disease or condition.
Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical: Statement of good health/free of communicable disease explanation and instruction: This 9 can be filled in electronically. ________________ i have examined _______________________________________, and to. I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable.
Statement of good health/free of communicable disease explanation and instruction: This 9 can be filled in electronically. I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Physician’s statement form date of physical: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. Complete the following information to notify the florida department of health of a reportable disease or condition. ________________ i have examined _______________________________________, and to.

Free Of Communicable Disease Form Captions Trend Today
Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Physician’s statement form date of physical: This 9 can be filled in.

Fillable Online COMMUNICABLE DISEASE GUIDELINE CHART FOR CHILD CARE
Statement of good health/free of communicable disease explanation and instruction: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical: This 9 can be filled.
Communicable Disease Screening Complete with ease airSlate SignNow
This 9 can be filled in electronically. Statement of good health/free of communicable disease explanation and instruction: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. ________________ i have examined _______________________________________, and to. I have examined the individual named above and to the best of my knowledge.
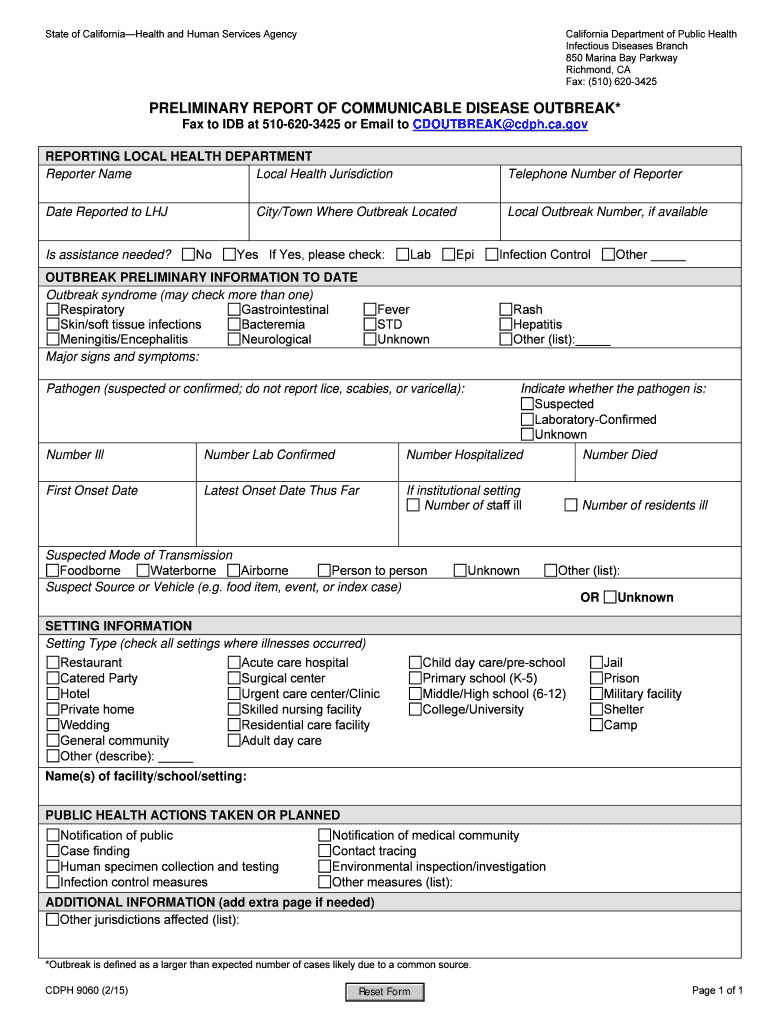
Fillable Online cdph ca Preliminary Report of Communicable Disease
Statement of good health/free of communicable disease explanation and instruction: Complete the following information to notify the florida department of health of a reportable disease or condition. This 9 can be filled in electronically. Physician’s statement form date of physical: ________________ i have examined _______________________________________, and to.
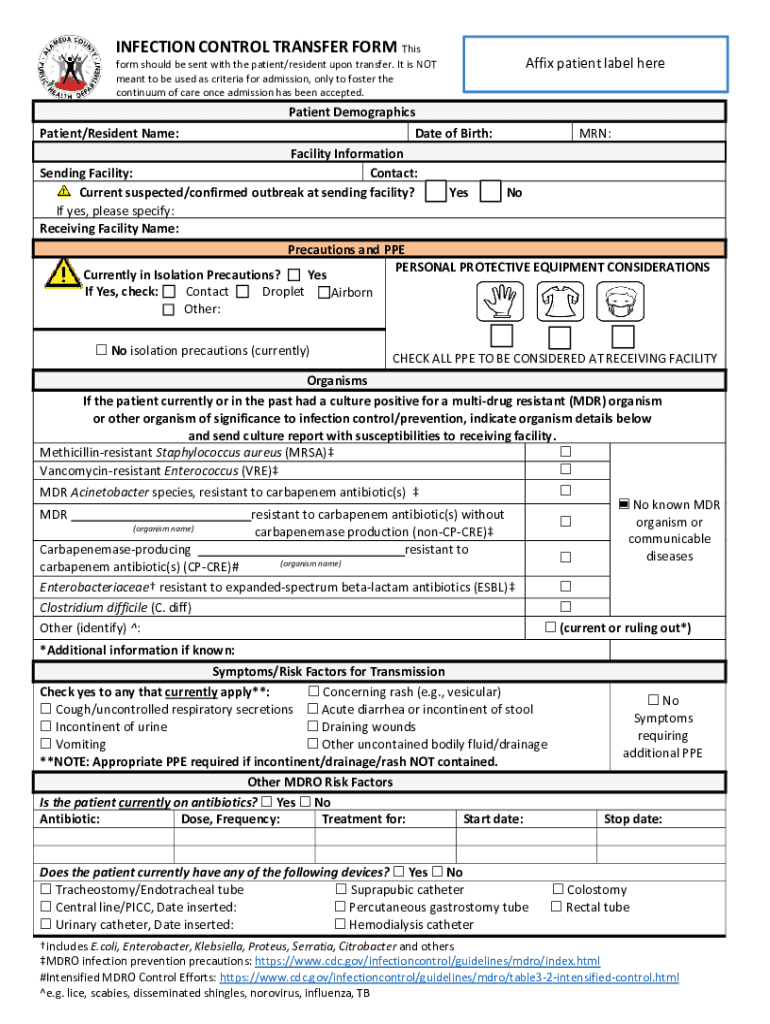
Fillable Online Division of Communicable Disease Control & Prevention
This 9 can be filled in electronically. ________________ i have examined _______________________________________, and to. Statement of good health/free of communicable disease explanation and instruction: Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical:

Free of communicable disease form Fill out & sign online DocHub
Statement of good health/free of communicable disease explanation and instruction: Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical: ________________ i have examined _______________________________________, and to. Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no.
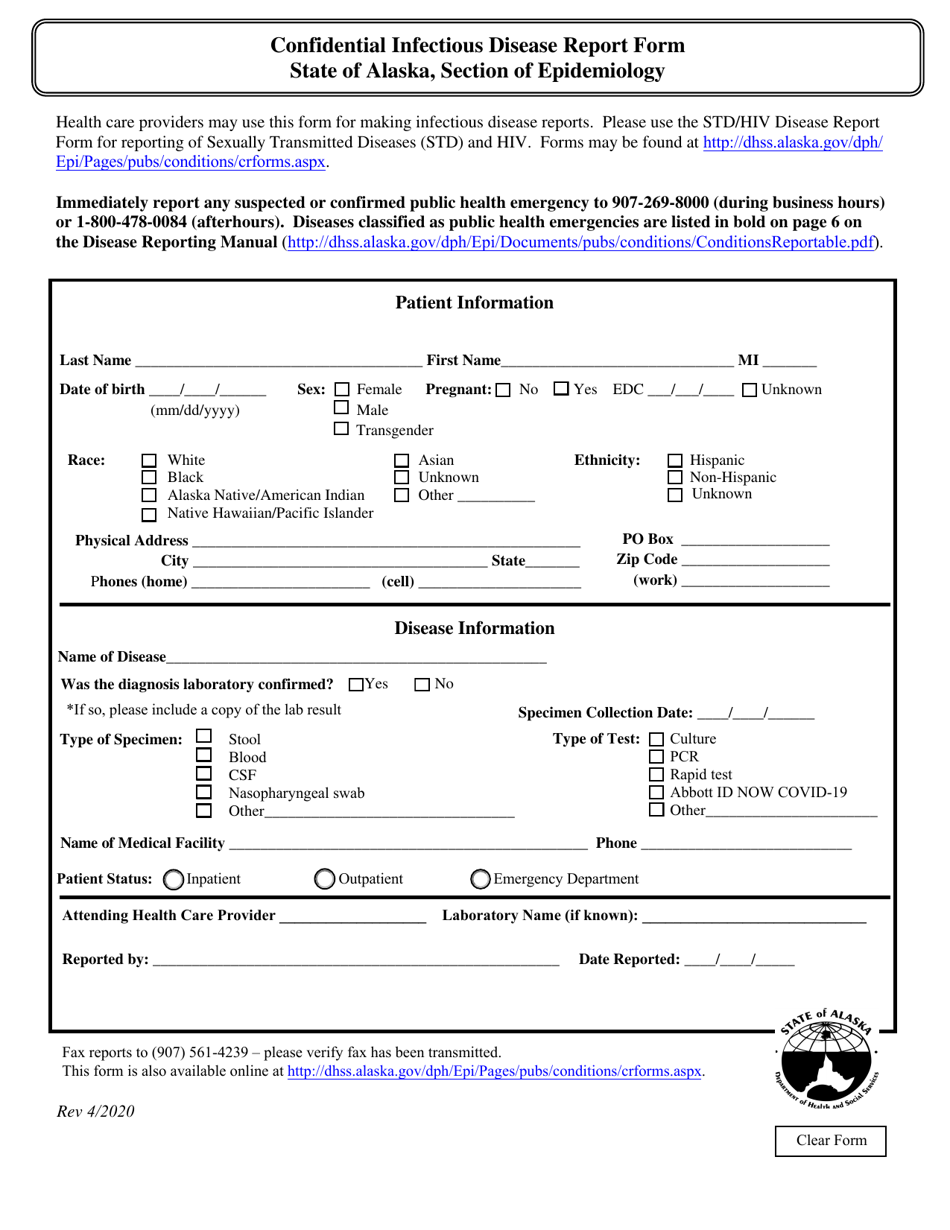
Alaska Confidential Infectious Disease Report Form Fill Out, Sign
I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. ________________ i have examined _______________________________________, and to. Complete the following information to notify the florida department of health of a reportable disease or condition. Patient name and he/she (circle one) appears to be free.
FREE 15+ Case Report Forms in PDF MS Word
Complete the following information to notify the florida department of health of a reportable disease or condition. ________________ i have examined _______________________________________, and to. Physician’s statement form date of physical: I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Patient name and he/she.
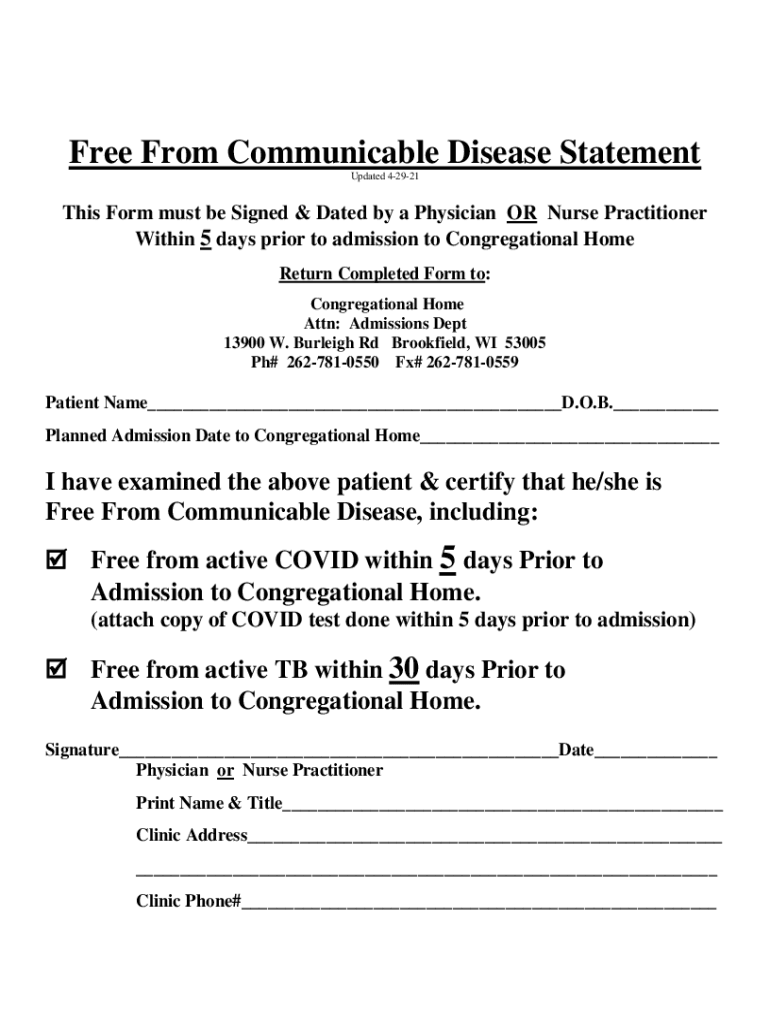
Fillable Online Free From Communicable Disease Statement Congregational
Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. ________________ i have examined _______________________________________, and to. Statement of good health/free of communicable disease explanation.
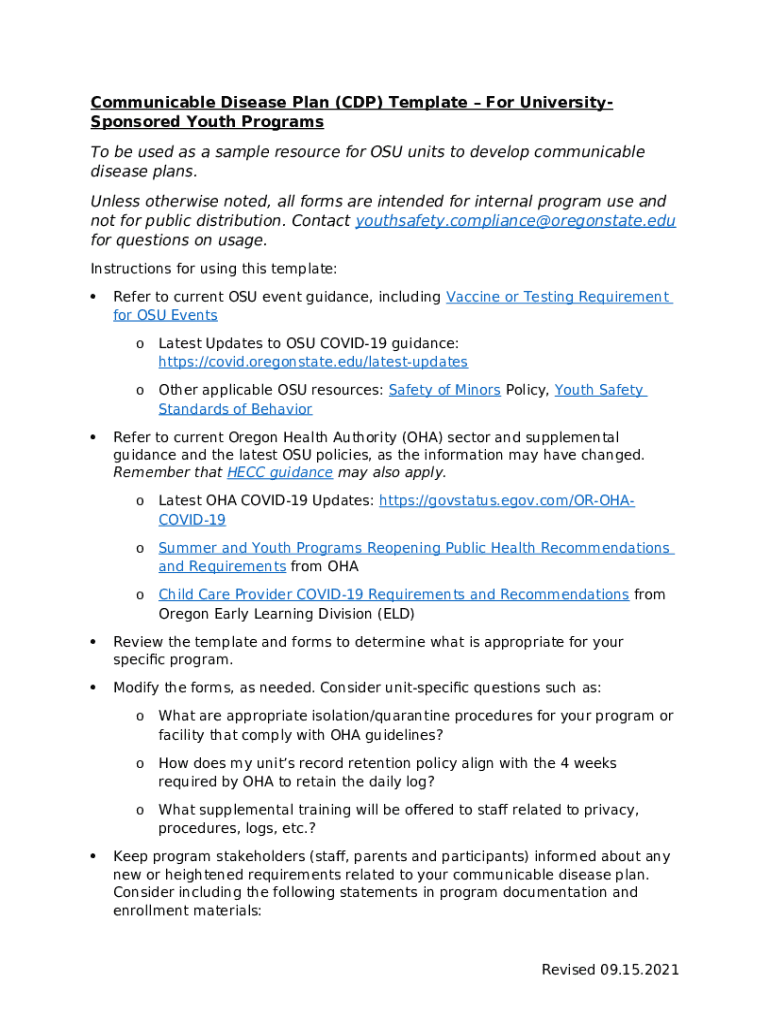
Communicable Disease Plan Template Doc Template pdfFiller
Complete the following information to notify the florida department of health of a reportable disease or condition. ________________ i have examined _______________________________________, and to. Physician’s statement form date of physical: Statement of good health/free of communicable disease explanation and instruction: This 9 can be filled in electronically.
Statement Of Good Health/Free Of Communicable Disease Explanation And Instruction:
I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Complete the following information to notify the florida department of health of a reportable disease or condition. Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. ________________ i have examined _______________________________________, and to.
This 9 Can Be Filled In Electronically.
Physician’s statement form date of physical: