Release Of Information Form Template Mental Health - I understand that any cancellation or modification of this authorization must be in. That my signing of this authorization is voluntary. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; Of my information as specified above. And/or hipaa 45 cfr) and state. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. By signing below, i authorize the release. I am giving my permission to compass health to disclose my confidential health records. I understand that i have a right to receive a copy of this authorization.
By signing below, i authorize the release. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. I am giving my permission to compass health to disclose my confidential health records. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; Of my information as specified above. I understand that i have a right to receive a copy of this authorization. That my signing of this authorization is voluntary. I understand that any cancellation or modification of this authorization must be in. And/or hipaa 45 cfr) and state.
By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. Of my information as specified above. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; By signing below, i authorize the release. And/or hipaa 45 cfr) and state. I understand that i have a right to receive a copy of this authorization. I am giving my permission to compass health to disclose my confidential health records. That my signing of this authorization is voluntary. I understand that any cancellation or modification of this authorization must be in.

Release Of Information Form Template Mental Health
By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. And/or hipaa 45 cfr) and state. I am giving my permission to compass health to disclose my confidential health records. I understand that any cancellation or modification of this authorization must be in. That my signing of this authorization.
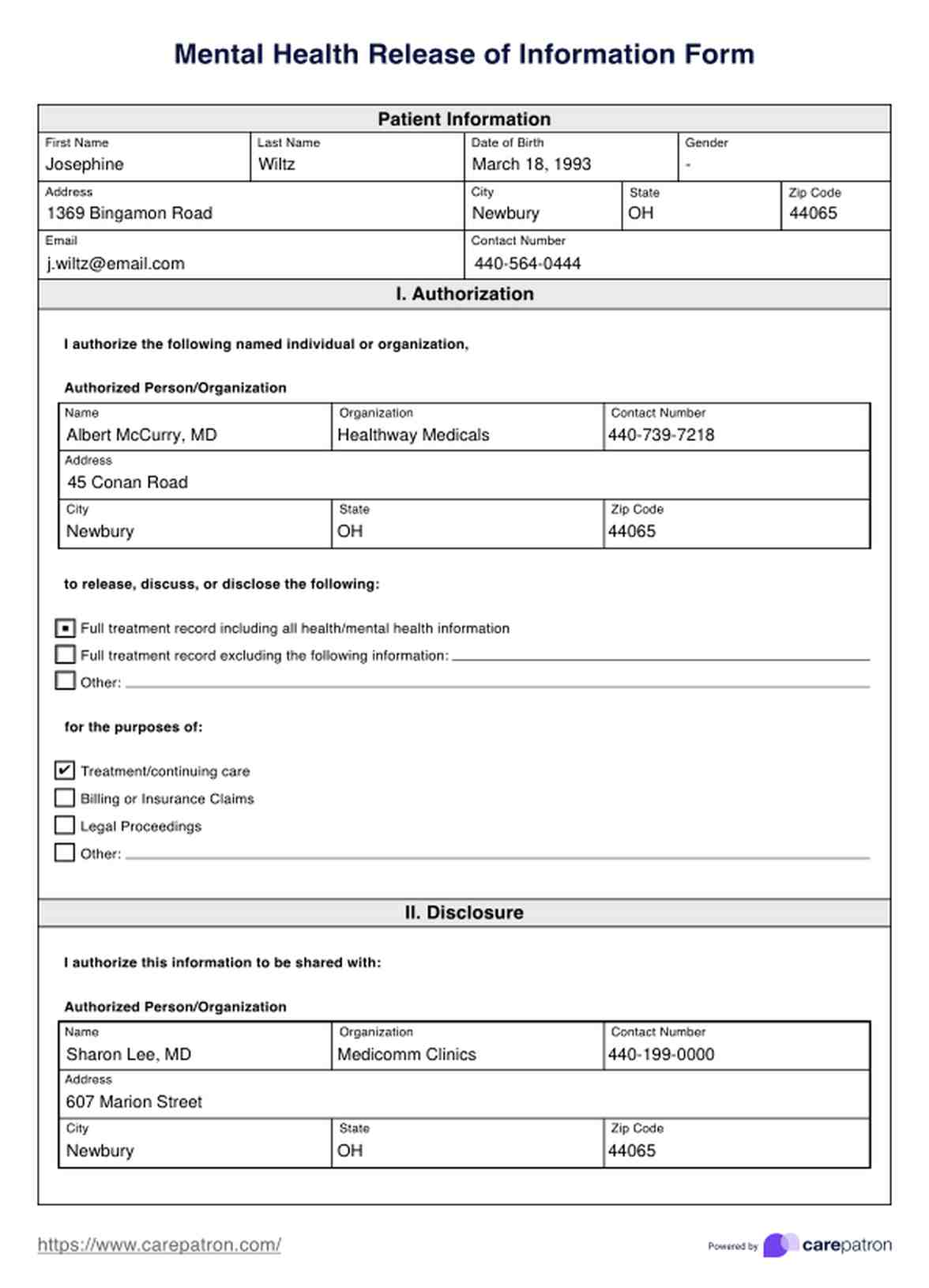
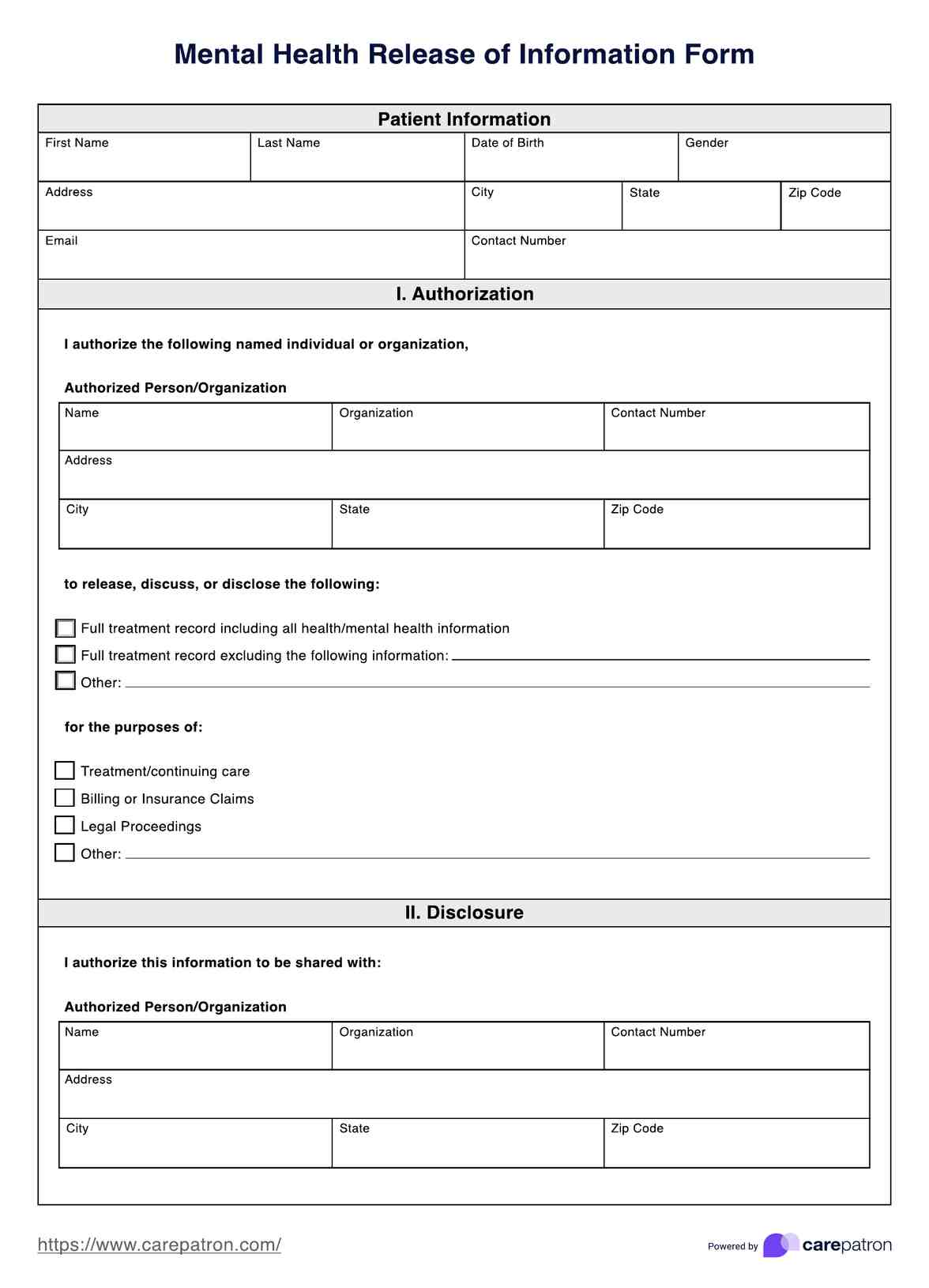
Mental Health Release Of Information Form & Template Free PDF Download
Of my information as specified above. That my signing of this authorization is voluntary. I understand that i have a right to receive a copy of this authorization. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. By signing below, i authorize the release.
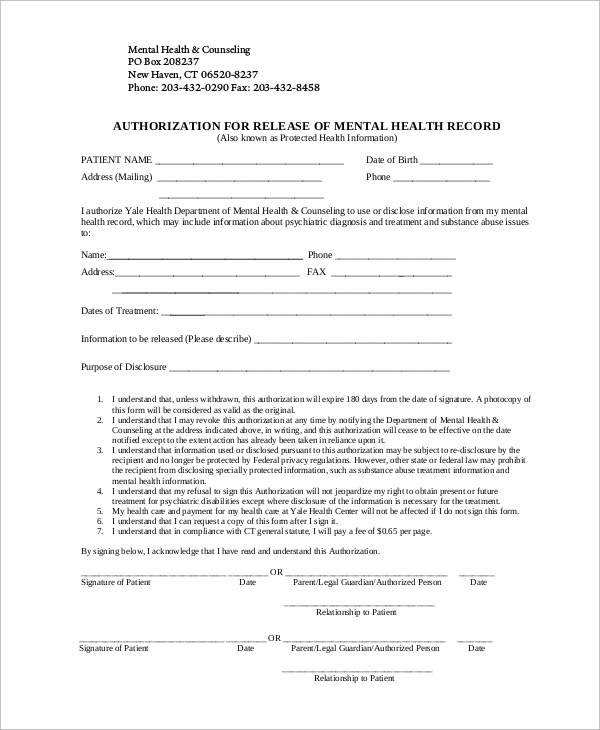
FREE 9+ Sample Release of Information Forms in MS Word PDF
I understand that any cancellation or modification of this authorization must be in. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I am giving my permission to compass health to disclose my confidential health records. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed.

Mental Health Release Of Information Form & Template Free PDF Download
I understand that any cancellation or modification of this authorization must be in. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. I understand that i have a right to receive a copy of this authorization. That my signing of this authorization is voluntary. My health.
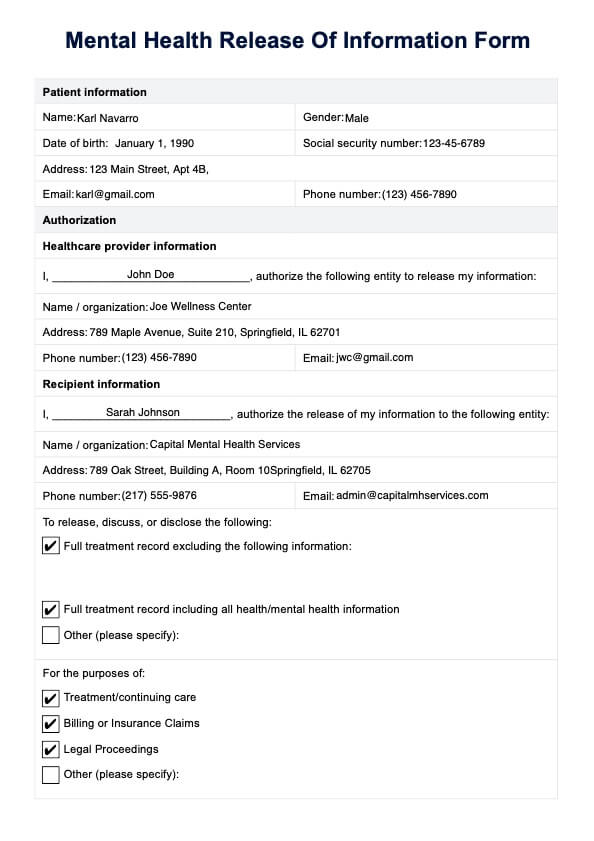
Mental Health Release of Information Form & Template Free PDF Download
I am giving my permission to compass health to disclose my confidential health records. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that any cancellation or modification of this authorization must be in. That my signing of this authorization is voluntary. I understand that i have a right.
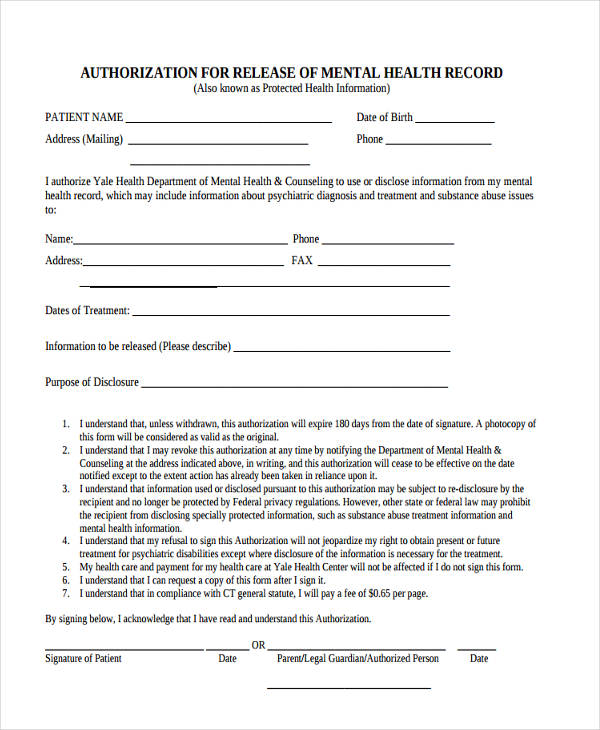
FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; That my signing of this authorization is voluntary. And/or hipaa 45 cfr) and state. I understand that i have a right to receive a copy of this authorization. By signing this form, confidential psychological and psychiatric information can be released to and/or.

Release Of Information Form Template Mental Health
By signing below, i authorize the release. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. I understand that i have a right to receive a copy of this authorization. I understand that any cancellation or modification of this authorization must be in. Of my information.
Release Of Information Form Template Mental Health
I understand that i have a right to receive a copy of this authorization. By signing below, i authorize the release. Of my information as specified above. I understand that any cancellation or modification of this authorization must be in. And/or hipaa 45 cfr) and state.

Mental Health Release Of Information Template
And/or hipaa 45 cfr) and state. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. By signing below, i authorize the release. I understand that i have a right to receive a copy of this authorization. My health information is protected by federal regulation (alcohol &.
Printable Mental Health Release Form
I am giving my permission to compass health to disclose my confidential health records. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. I understand that i have a right to receive a copy of this authorization. This template can be used to coordinate the release of confidential.
My Health Information Is Protected By Federal Regulation (Alcohol & Drug Abuse Patient Records, 42 Cfr Part 2;
That my signing of this authorization is voluntary. Of my information as specified above. By signing below, i authorize the release. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private.
I Understand That I Have A Right To Receive A Copy Of This Authorization.
By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. I understand that any cancellation or modification of this authorization must be in. And/or hipaa 45 cfr) and state. I am giving my permission to compass health to disclose my confidential health records.