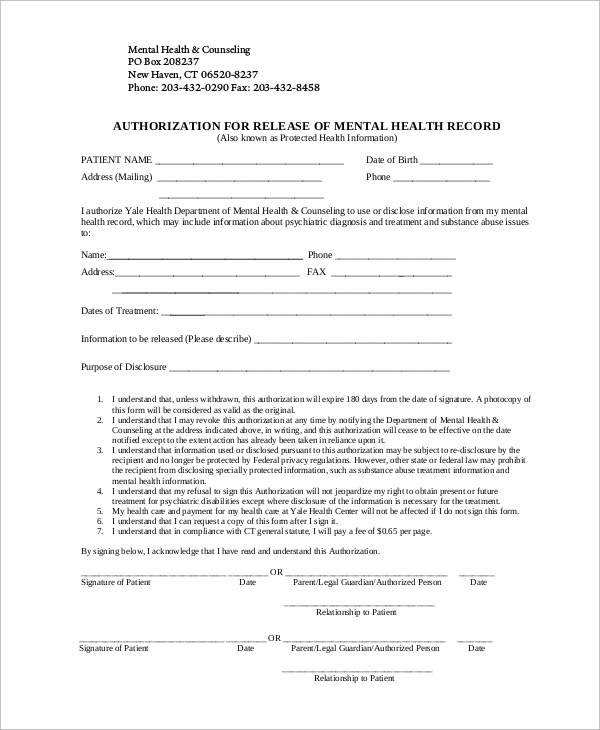
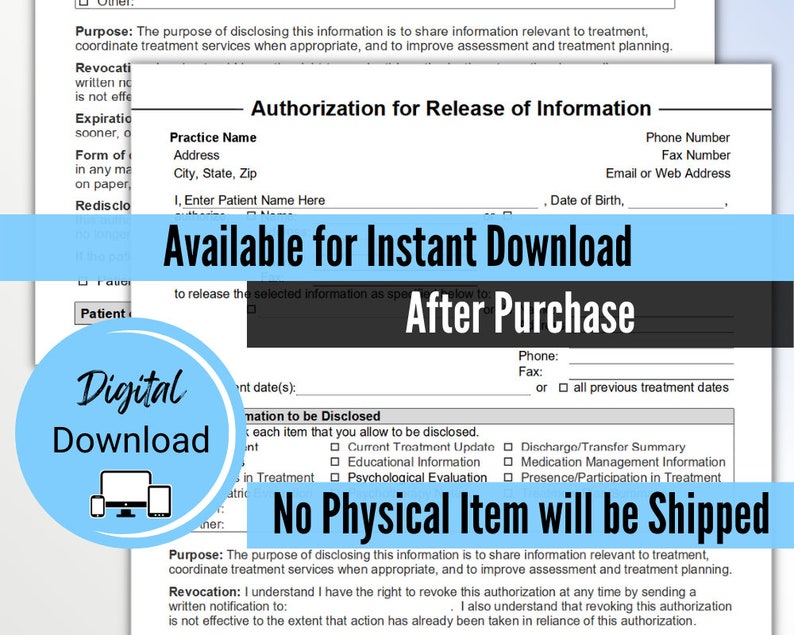
Release Of Information Template For Mental Health - That my signing of this authorization is voluntary. By signing below, i authorize the release. I am giving my permission to compass health to disclose my confidential health records. And/or hipaa 45 cfr) and state. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. And/or hipaa 45 cfr) and state. Of my information as specified above.
Of my information as specified above. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. I am giving my permission to compass health to disclose my confidential health records. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; And/or hipaa 45 cfr) and state. By signing below, i authorize the release. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; And/or hipaa 45 cfr) and state. That my signing of this authorization is voluntary.
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. I am giving my permission to compass health to disclose my confidential health records. And/or hipaa 45 cfr) and state. Of my information as specified above. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; By signing below, i authorize the release. And/or hipaa 45 cfr) and state. That my signing of this authorization is voluntary.
Release Of Information Form Template Mental Health
Of my information as specified above. And/or hipaa 45 cfr) and state. I am giving my permission to compass health to disclose my confidential health records. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr.
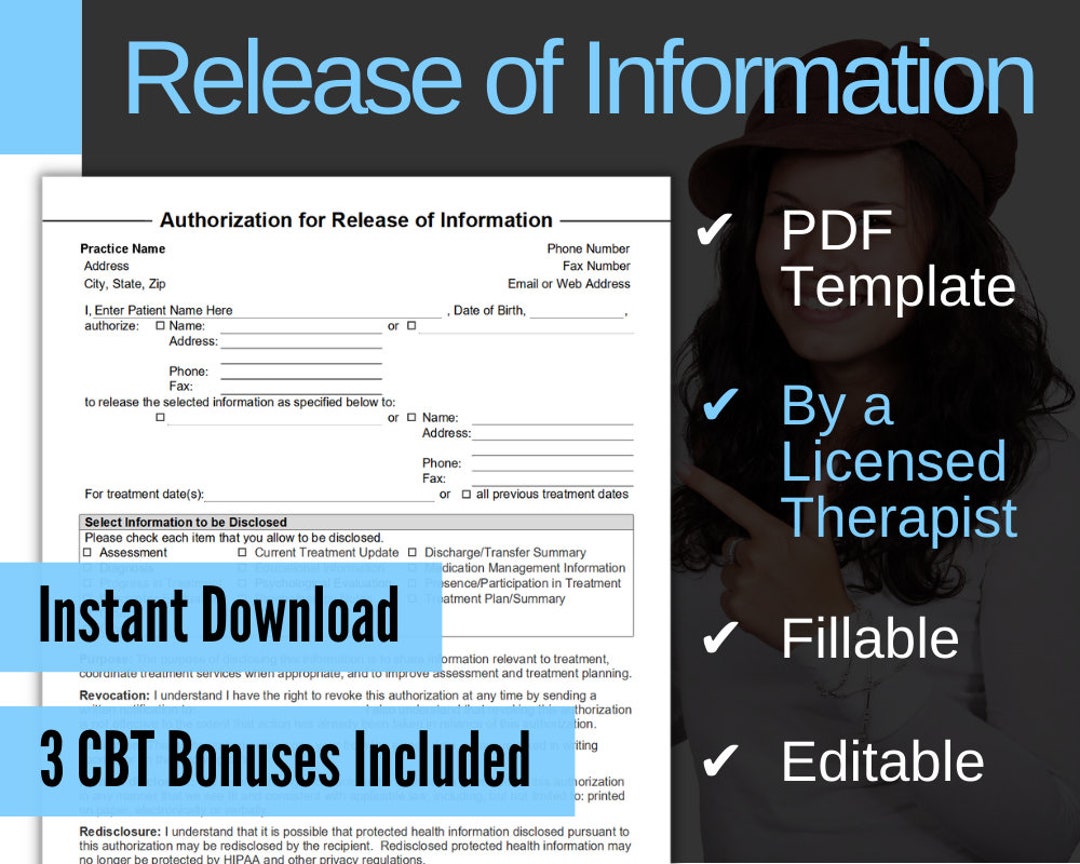
Mental Health Release of Information Form, ROI, PDF, Fillable, Editable
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; And/or hipaa 45 cfr) and state. And/or hipaa 45 cfr) and state. That my signing of this authorization is voluntary.
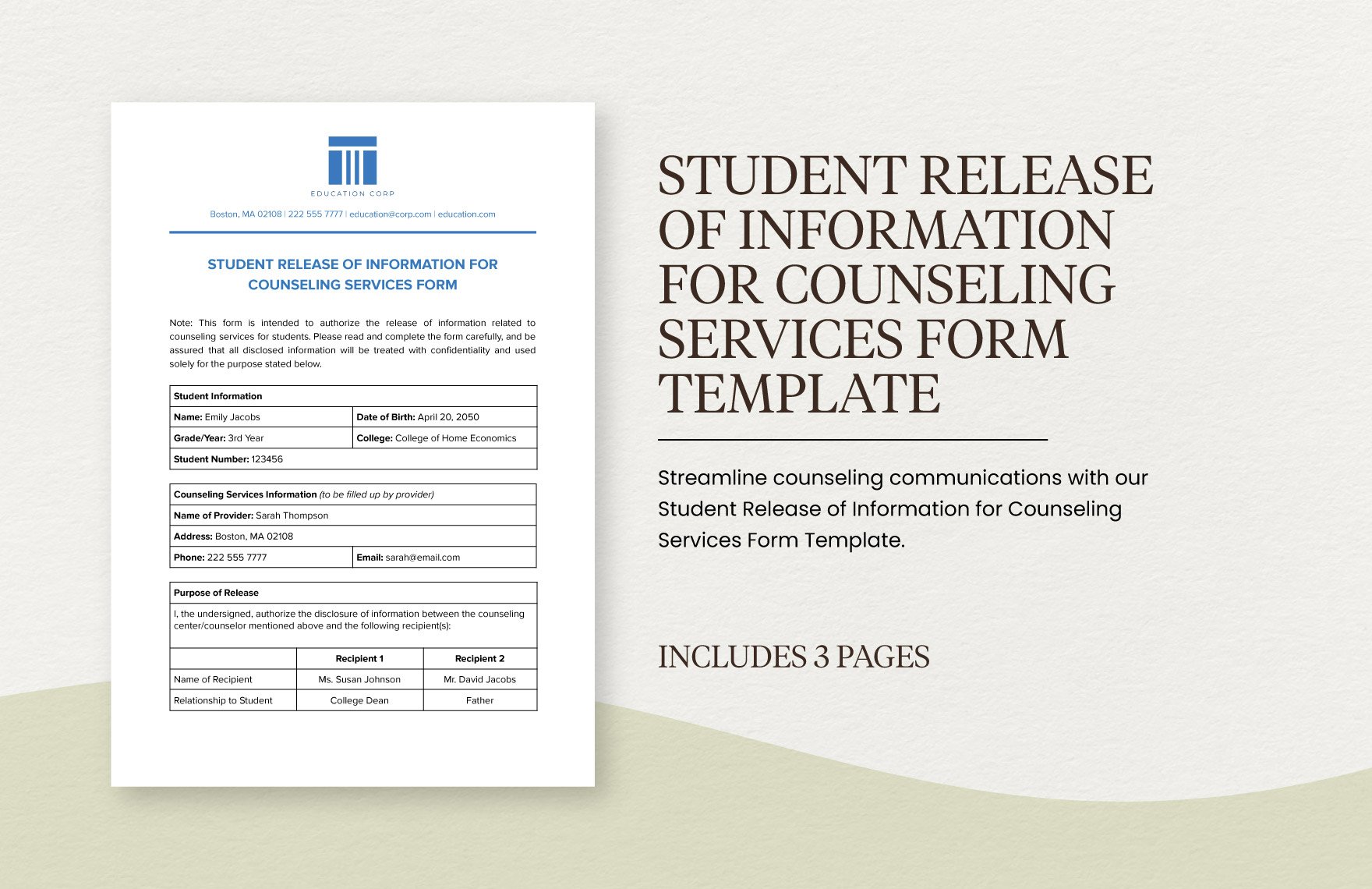
Editable Student Form Templates in PDF to Download
And/or hipaa 45 cfr) and state. Of my information as specified above. And/or hipaa 45 cfr) and state. That my signing of this authorization is voluntary. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,.

Mental Health Release Of Information Form & Template Free PDF Download
And/or hipaa 45 cfr) and state. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; That my signing of this authorization is voluntary. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. I am giving my permission to compass.
Mental Health Release of Information Form, ROI, PDF, Fillable, Editable
And/or hipaa 45 cfr) and state. I am giving my permission to compass health to disclose my confidential health records. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. By signing below, i authorize the release. My health information is protected by federal regulation (alcohol & drug abuse.
FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
And/or hipaa 45 cfr) and state. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; That my signing of this authorization is voluntary. I am giving my permission to compass health to disclose my confidential health records. Of my information as specified above.
Release Of Information Form Mental Health Template
And/or hipaa 45 cfr) and state. And/or hipaa 45 cfr) and state. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. I am giving my permission to compass health to disclose my confidential health records. Of my information as specified above.
Release Of Information Form Template Mental Health
I am giving my permission to compass health to disclose my confidential health records. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; And/or hipaa 45 cfr) and state. I understand that my.
Release of Info Mental Health ROI Privacy Paperwork Release of
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; By signing below, i authorize the release. And/or hipaa 45 cfr) and state. Of my information as specified above.
Free Release Of Information Form Mental Health Template Doc
By signing below, i authorize the release. Of my information as specified above. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. And/or hipaa 45 cfr) and state.
By Signing Below, I Authorize The Release.
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I am giving my permission to compass health to disclose my confidential health records.
And/Or Hipaa 45 Cfr) And State.
Of my information as specified above. And/or hipaa 45 cfr) and state. That my signing of this authorization is voluntary.