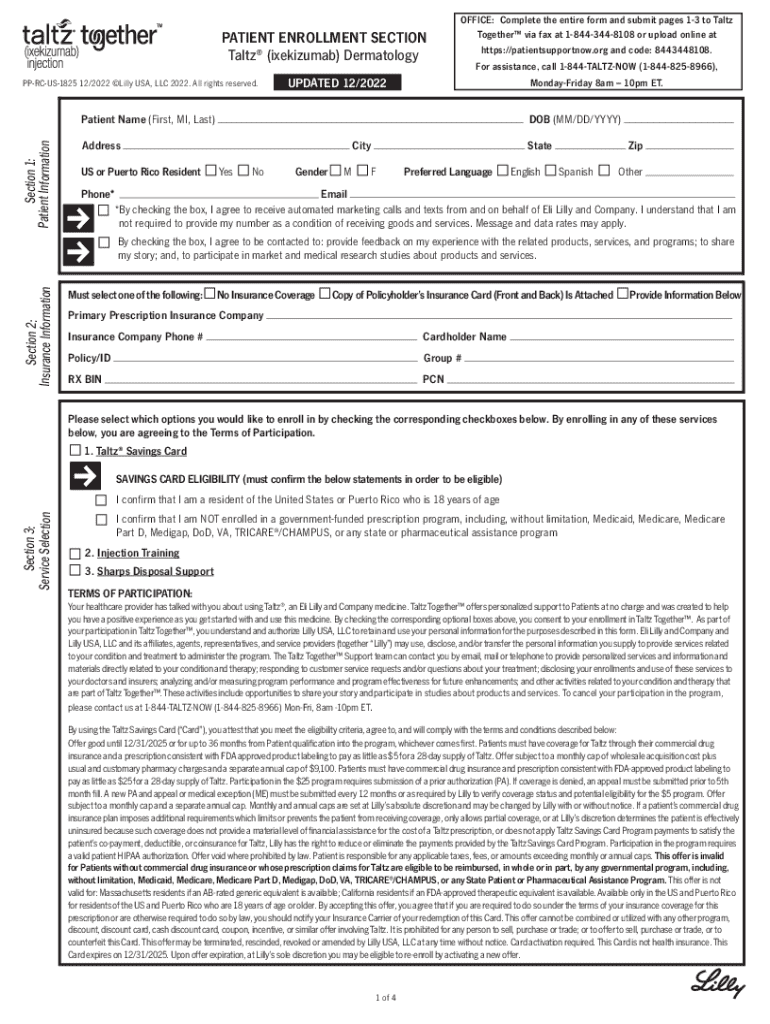
Taltz Enrollment Form - As part of your participation in lilly support servicestm for taltz®, you understand and authorize lilly usa, llc to retain and use your. I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. I understand that by signing this form, i am requesting support from eli lilly and company for patients receiving taltz® pursuant to an fda. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility.
As part of your participation in lilly support servicestm for taltz®, you understand and authorize lilly usa, llc to retain and use your. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. I understand that by signing this form, i am requesting support from eli lilly and company for patients receiving taltz® pursuant to an fda.
I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. As part of your participation in lilly support servicestm for taltz®, you understand and authorize lilly usa, llc to retain and use your. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. I understand that by signing this form, i am requesting support from eli lilly and company for patients receiving taltz® pursuant to an fda.

Fillable Online Taltz Together Pediatric Savings and Support Enrollment
By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. As part of your participation in lilly support servicestm for taltz®, you.
Fillable Online taltzenrollmentform.pdf Eli Lilly Fax Email Print
As part of your participation in lilly support servicestm for taltz®, you understand and authorize lilly usa, llc to retain and use your. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. I understand that by signing this form, i authorize my doctors, my healthcare plan.

Taltz Enrollment Form Download Fillable Start Form PDF
I understand that by signing this form, i am requesting support from eli lilly and company for patients receiving taltz® pursuant to an fda. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. As part of your participation in lilly support servicestm for taltz®, you understand.
Fillable Online Taltz Together Enrollment FormsTaltz (ixekizumab) Fax
I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. I understand that by signing this form, i am requesting support from.
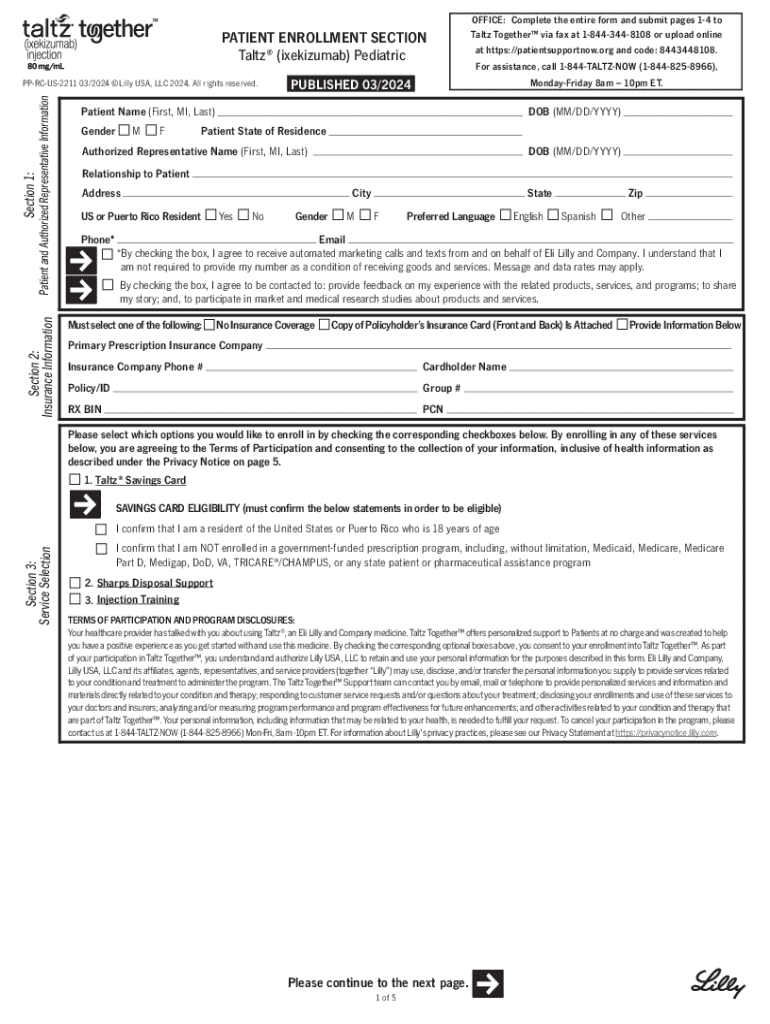
Fillable Online taltzpediatricenrollmentform.pdf Fax Email Print
I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. I understand that by signing this form, i am requesting support from.
Fillable Online Taltz Form Fax Email Print pdfFiller
By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. As part of your participation in lilly support servicestm for taltz®, you understand and authorize lilly usa, llc to retain and use your. I understand that by signing this form, i am requesting support from eli lilly.

Fillable Online Taltz Together Savings and Support Enrollment Form, and
I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. As part of your participation in lilly support servicestm for taltz®, you understand and authorize lilly usa, llc to retain and use your. I understand that by signing this form, i am requesting support from.

taltzenrollmentform PDF Medical Prescription Pharmacy
I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. As part of your participation in lilly support servicestm for taltz®, you.

Taltz Together Enrollment Form Fill Online, Printable, Fillable
As part of your participation in lilly support servicestm for taltz®, you understand and authorize lilly usa, llc to retain and use your. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. I understand that by signing this form, i am requesting support from eli lilly.

Taltz (ixekizumab) LillyPlus PSP Form 2021 World OSCAR
I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my. By enrolling in the taltz savings card program (“program”) and using the taltz savings card (“card”), you attest that you meet the eligibility. I understand that by signing this form, i am requesting support from.
By Enrolling In The Taltz Savings Card Program (“Program”) And Using The Taltz Savings Card (“Card”), You Attest That You Meet The Eligibility.
As part of your participation in lilly support servicestm for taltz®, you understand and authorize lilly usa, llc to retain and use your. I understand that by signing this form, i am requesting support from eli lilly and company for patients receiving taltz® pursuant to an fda. I understand that by signing this form, i authorize my doctors, my healthcare plan or insurance company, my pharmacies, or others who might hold my.