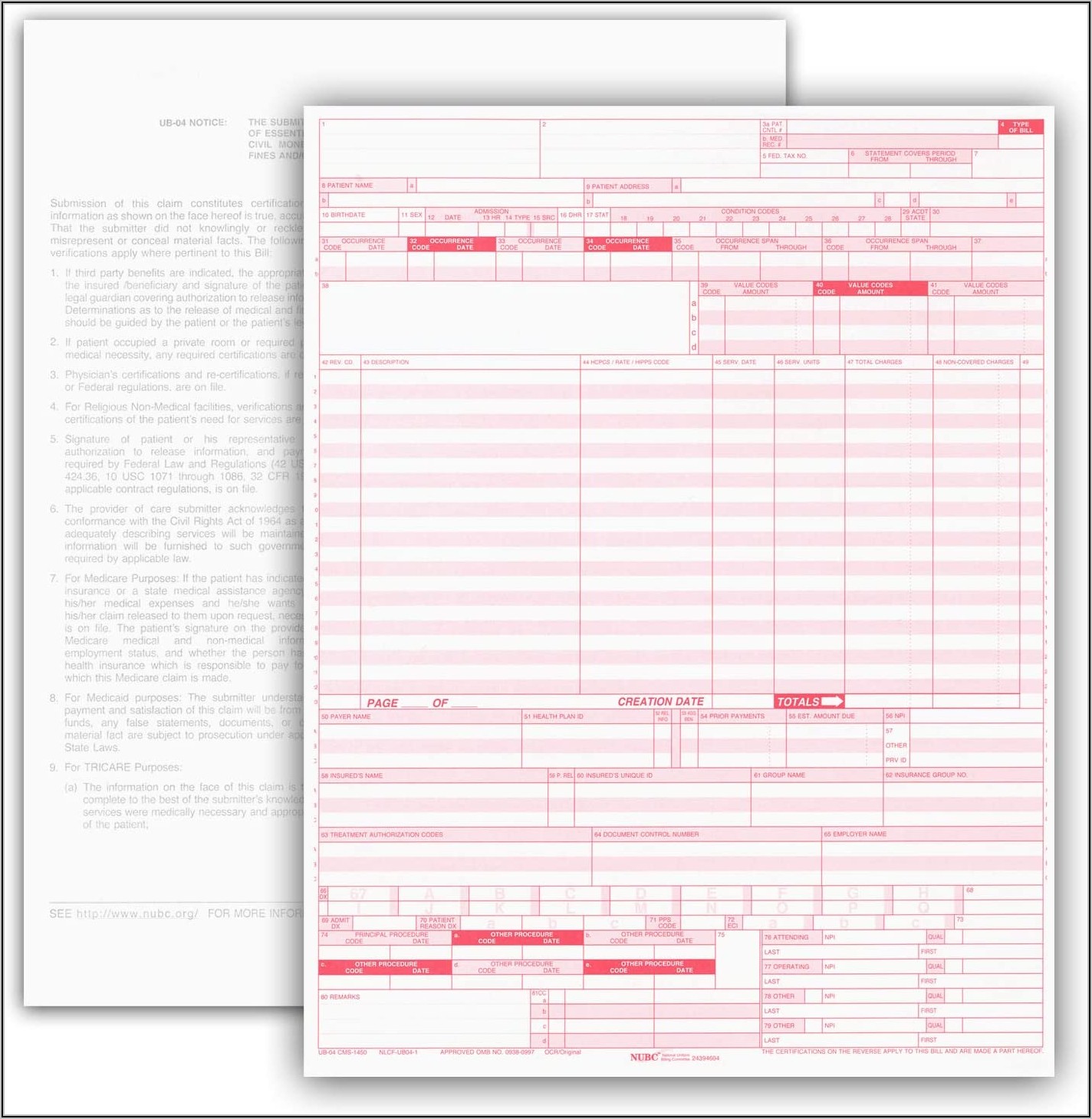
Ub04 Claim Form - Enter the name and address of the hospital/facility submitting the claim. Pay to address if different than field 1.
Enter the name and address of the hospital/facility submitting the claim. Pay to address if different than field 1.
Enter the name and address of the hospital/facility submitting the claim. Pay to address if different than field 1.
/UB04-57a5d9773df78cf459cd0ef3.jpg)
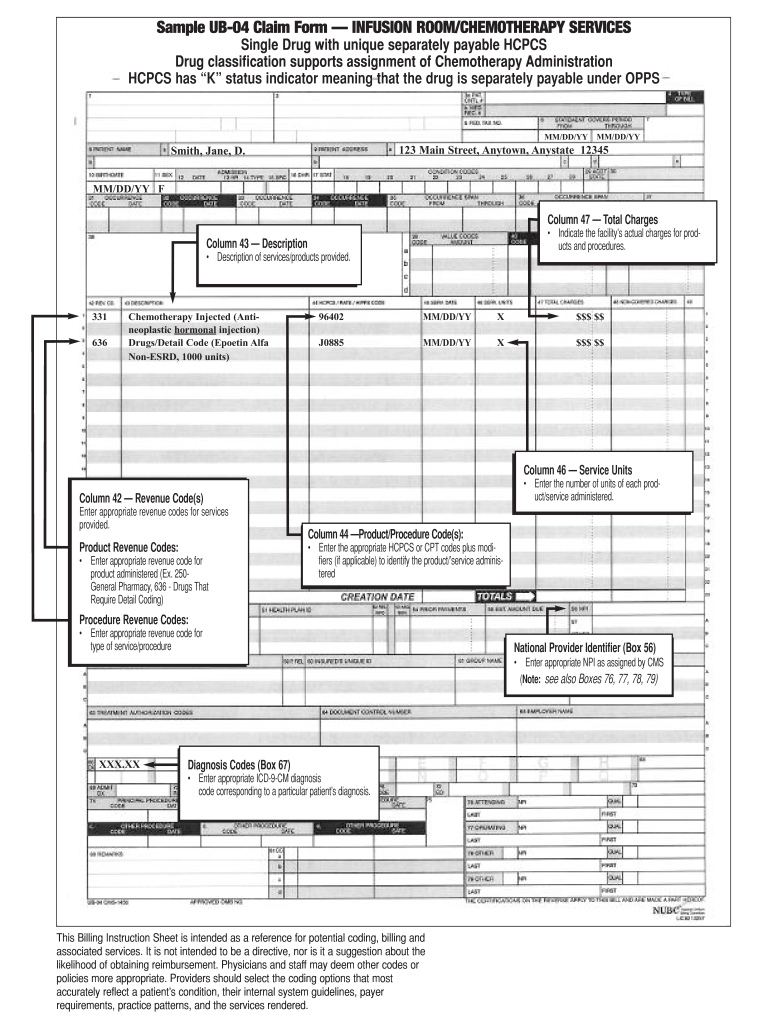
Overview of the UB04 Billing Claim Form
Pay to address if different than field 1. Enter the name and address of the hospital/facility submitting the claim.

500 UB04 Claim Forms, CMS 1450 Health Insurance Claim Forms for
Enter the name and address of the hospital/facility submitting the claim. Pay to address if different than field 1.

Fillable Online SAMPLE UB04 CLAIM FORM Fax Email Print pdfFiller
Enter the name and address of the hospital/facility submitting the claim. Pay to address if different than field 1.

What Is A Hospital Claim Form Called at Frank Thill blog
Enter the name and address of the hospital/facility submitting the claim. Pay to address if different than field 1.

Printable Ub04 Form Sample
Pay to address if different than field 1. Enter the name and address of the hospital/facility submitting the claim.
Printable Ub04 Form Sample Printable Templates
Pay to address if different than field 1. Enter the name and address of the hospital/facility submitting the claim.

UB04 Claim Form, CMS1450 Hospital Claim Form, 81/2 x 11" Pack of 500
Enter the name and address of the hospital/facility submitting the claim. Pay to address if different than field 1.
Ub04 Form Example Fill Online, Printable, Fillable, Blank pdfFiller
Pay to address if different than field 1. Enter the name and address of the hospital/facility submitting the claim.

Ub 04 Claim Form Printable Printable Forms Free Online
Enter the name and address of the hospital/facility submitting the claim. Pay to address if different than field 1.
Printable Ub 04 Claim Form Printable Forms Free Online
Pay to address if different than field 1. Enter the name and address of the hospital/facility submitting the claim.
Enter The Name And Address Of The Hospital/Facility Submitting The Claim.
Pay to address if different than field 1.